de Oliveira Andrade Matheus, Felix Vitor Hugo, Testa Laura, Bonadioa Renata Colombo
Instituto do Câncer do Estado de São Paulo (ICESP), Faculdade de Medicina da Universidade de São Paulo (FMUSP), São Paulo 01246-000, Brazil.
https://orcid.org/0000-0001-5818-922X.
Ecancermedicalscience. 2025 Apr 17;19:1894. doi: 10.3332/ecancer.2025.1894. eCollection 2025.
Visceral crisis (VC) in metastatic breast cancer (MBC) is defined as a severe organ dysfunction related to metastatic disease. The cornerstone of treatment for VC relies on polychemotherapy, particularly in low- and middle-income countries, where it often represents the only available therapeutic option. This study aims to assess survival outcomes of palliative chemotherapy (CT) for VC in a real-world scenario.
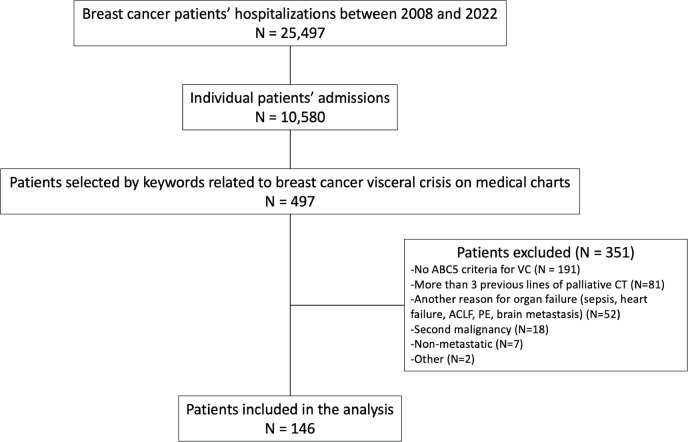
Data were retrospectively collected from patients with MBC diagnosed with VC between 2008 and 2022 in a large cancer center in Brazil. Survival analyses were performed using the Kaplan-Meier method. Prognostic factors were evaluated through univariate and multivariable analyses using the Cox regression model.
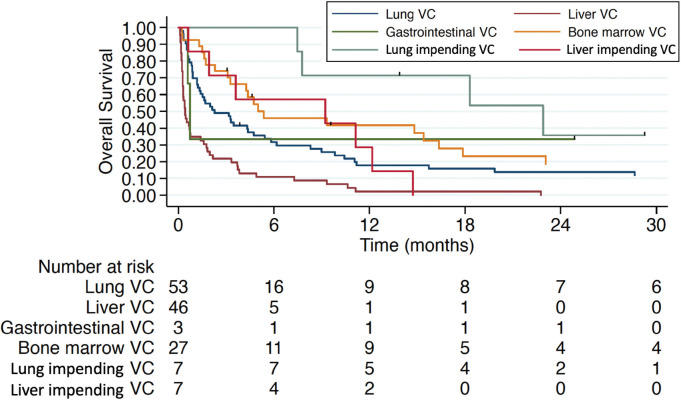
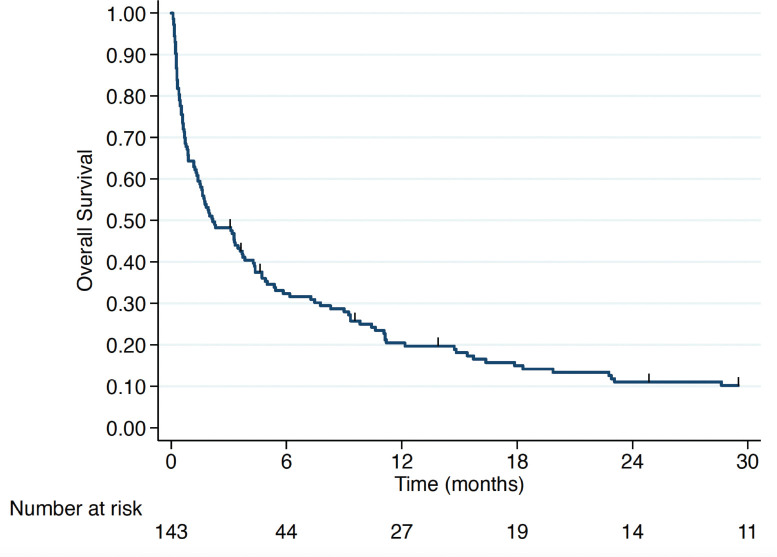
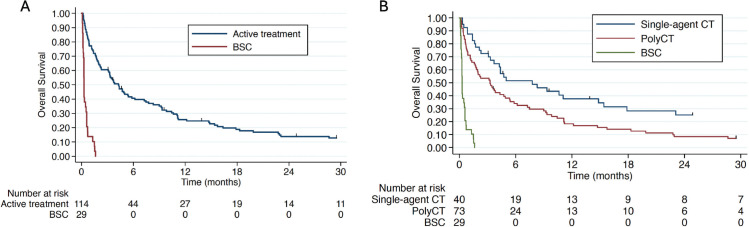
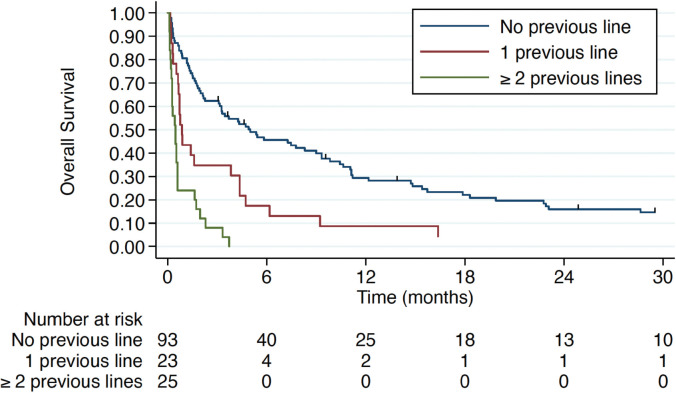
A total of 146 patients with VC were included. The predominant type of VC was pulmonary (36.3%), hepatic (32.2%) and bone marrow infiltration (19.2%). VC management was based on combination CT (51.4%), while 27.4% were treated with monochemotherapy and 20.6% received best supportive care (BSC). The median overall survival (mOS) for the entire population was 2.17 months. Treatment for VC in the first-line setting was associated with a mOS of 5 months. In the multivariate analysis, hepatic VC and the absence of active oncological therapy (BSC) were significantly associated with mortality.
Patients with MBC in VC have a poor prognosis even when treated with polychemotherapy. Proper prognostication is crucial for identifying patients who may benefit from active systemic therapy while carefully avoiding potentially futile strategies. Prospective trials including patients with VC criteria are needed to evaluate the efficacy and safety of CT and other emerging therapies in this scenario.
转移性乳腺癌(MBC)中的内脏危机(VC)被定义为与转移性疾病相关的严重器官功能障碍。VC治疗的基石依赖于多药化疗,尤其是在低收入和中等收入国家,多药化疗往往是唯一可用的治疗选择。本研究旨在评估在现实世界中姑息化疗(CT)治疗VC的生存结果。
回顾性收集2008年至2022年期间在巴西一家大型癌症中心诊断为VC的MBC患者的数据。使用Kaplan-Meier方法进行生存分析。通过使用Cox回归模型的单变量和多变量分析来评估预后因素。
共纳入146例VC患者。VC的主要类型为肺部(36.3%)、肝脏(32.2%)和骨髓浸润(19.2%)。VC的管理基于联合CT(占51.4%),而27.4%接受单药化疗,20.6%接受最佳支持治疗(BSC)。整个人群的中位总生存期(mOS)为2.17个月。一线治疗VC的mOS为5个月。在多变量分析中,肝脏VC和无积极的肿瘤治疗(BSC)与死亡率显著相关。
即使接受多药化疗,MBC合并VC的患者预后也较差。正确的预后评估对于识别可能从积极的全身治疗中获益的患者至关重要,同时要谨慎避免潜在的无效策略。需要开展包括符合VC标准患者的前瞻性试验,以评估CT和其他新兴疗法在这种情况下的疗效和安全性。