Department of Anesthesiology, Vagelos College of Physicians and Surgeons, New York, New York.
Department of Health Policy and Management, Columbia Mailman School of Public Health, New York, New York.
Anesthesiology. 2023 Dec 1;139(6):734-745. doi: 10.1097/ALN.0000000000004743.
Labor neuraxial analgesia may reduce the odds of postpartum hemorrhage, the leading indication for maternal blood transfusion during childbirth. This study tested the hypothesis that labor neuraxial analgesia is associated with reduced odds of maternal blood transfusion overall.
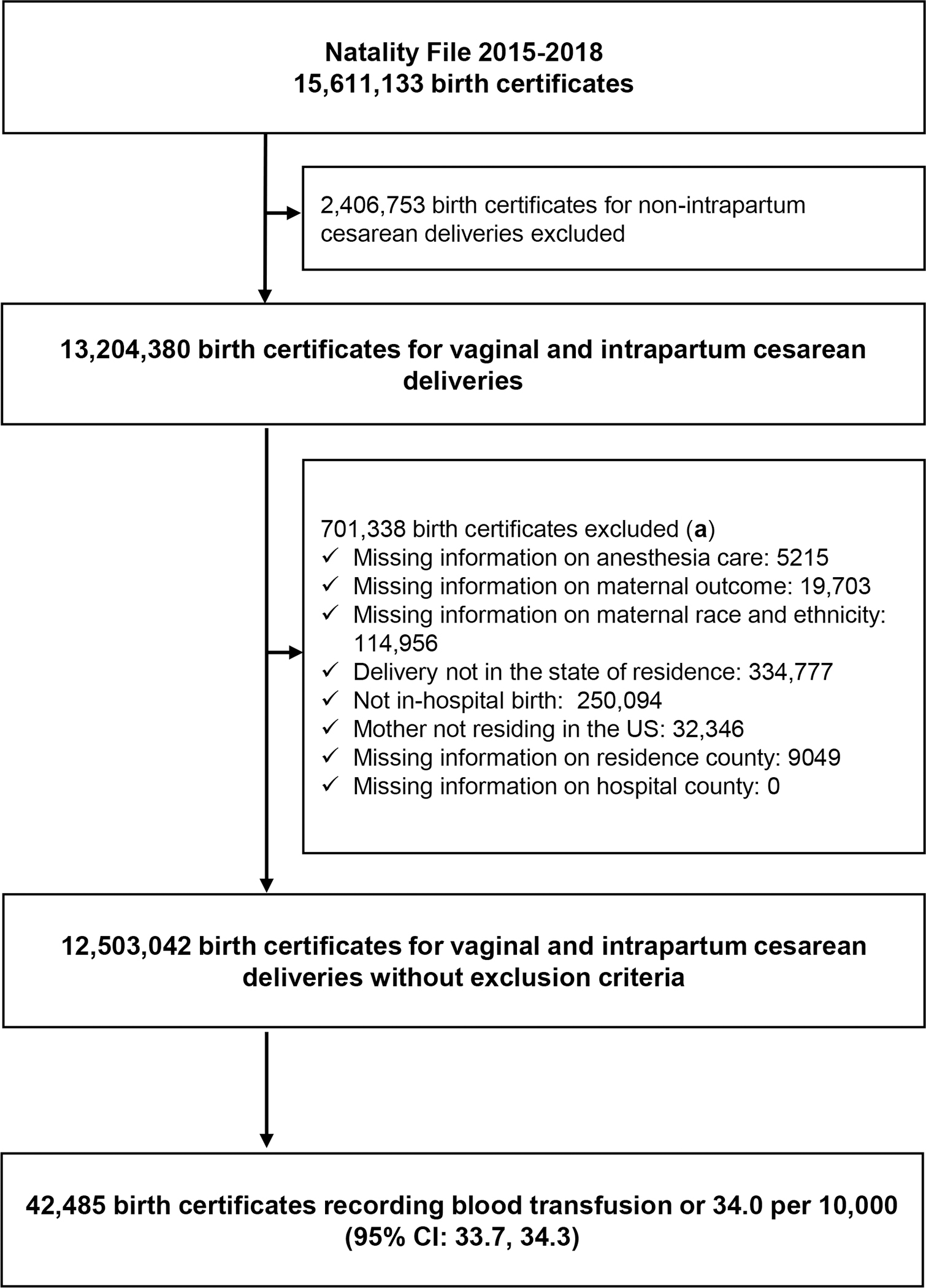
U.S. birth certificate data in the Natality File of the National Vital Statistics System for all 50 states from 2015 to 2018 for vaginal and intrapartum cesarean deliveries were analyzed. The exposure was labor neuraxial analgesia. The primary outcome was maternal blood transfusion, recorded on the birth certificate, which has low sensitivity for this outcome. Adjusted odds ratios and 95% CIs of blood transfusion associated with neuraxial analgesia were estimated using propensity score matching. The adjusted odds ratios were estimated overall and according to delivery mode, and treatment effect was compared between vaginal and intrapartum cesarean deliveries using an interaction term. Sensitivity analyses were performed using inverse propensity score weighting and quantitative bias analysis for outcome misclassification.
Of the 12,503,042 deliveries analyzed, 9,479,291 (75.82%) were with neuraxial analgesia, and 42,485 (0.34%) involved maternal blood transfusion. After propensity score matching, the incidence of blood transfusion was 0.30% in women without neuraxial analgesia (7,907 of 2,589,493) and 0.20% in women with neuraxial analgesia (5,225 of 2,589,493), yielding an adjusted odds ratio of 0.87 (95% CI, 0.82 to 0.91) overall. For intrapartum cesarean deliveries, the adjusted odds ratio was 0.55 (95% CI, 0.48 to 0.64), and for vaginal deliveries it was 0.93 (95% CI,. 0.88 to 0.98; P value for the interaction term < 0.001). The results were consistent in the sensitivity analyses, although the quantitative bias analysis demonstrated wide variation in potential effect size point estimates.
Labor neuraxial analgesia may be associated with reduced odds of maternal blood transfusion in intrapartum cesarean deliveries and, to a lesser extent, vaginal deliveries. The specific effect size varies widely by delivery mode and is unclear given the poor sensitivity of the data set for the maternal transfusion primary outcome.
分娩时使用椎管内镇痛可以降低产后出血的几率,产后出血是分娩期间产妇输血的主要指征。本研究检验了这样一个假设,即分娩时使用椎管内镇痛总体上与降低产妇输血的几率有关。
分析了 2015 年至 2018 年美国全国生命统计系统生育档案中来自 50 个州的所有阴道分娩和产时剖宫产分娩的出生证明数据。暴露因素是分娩时使用椎管内镇痛。主要结局是记录在出生证明上的产妇输血,该数据对这一结局的敏感性较低。使用倾向评分匹配法估计与椎管内镇痛相关的输血的校正比值比和 95%置信区间。总体上以及根据分娩方式估计校正比值比,并使用交互项比较阴道分娩和产时剖宫产之间的治疗效果。使用逆倾向评分加权和定量偏倚分析进行结局误分类的敏感性分析。
在分析的 12503042 次分娩中,9479291 次(75.82%)使用了椎管内镇痛,42485 次(0.34%)涉及产妇输血。在进行倾向评分匹配后,未使用椎管内镇痛的女性输血发生率为 0.30%(7907/2589493),使用椎管内镇痛的女性输血发生率为 0.20%(5225/2589493),校正比值比为 0.87(95%CI,0.82 至 0.91)。对于产时剖宫产,校正比值比为 0.55(95%CI,0.48 至 0.64),对于阴道分娩,校正比值比为 0.93(95%CI,0.88 至 0.98;交互项 P 值<0.001)。敏感性分析结果一致,尽管定量偏倚分析表明潜在效应大小点估计值存在广泛差异。
分娩时使用椎管内镇痛可能与产时剖宫产以及在一定程度上与阴道分娩时产妇输血的几率降低有关。由于数据集对产妇输血主要结局的敏感性较低,因此特定的效应大小因分娩方式而异,尚不清楚。