Department of Head and Neck Surgery, Sichuan Cancer Hospital & Institute, Sichuan Cancer Center, University of Electronic Science and Technology of China, , Chengdu, China.
Department of Head and Neck Surgery, Education & Training, Sichuan Cancer Center, University of Electronic Science and Technology of China, Chengdu, China.
World J Surg Oncol. 2023 Aug 17;21(1):249. doi: 10.1186/s12957-023-03075-w.
To explore relevant clinical factors of level IIB and contralateral level VI lymph node metastasis and evaluate the safety of low-collar extended incision (LCEI) for lymph node dissection in level II for papillary thyroid carcinoma (PTC) with pN1b.
A retrospective analysis was performed on 218 patients with PTC with pN1b who were treated surgically in the Head and Neck Surgery Center of Sichuan Cancer Hospital from September 2021 to May 2022. Data on age, sex, body mass index (BMI), tumor location, maximum tumor diameter, multifocality, Braf gene, T staging, surgical incision style, and lymph node metastasis in each cervical subregion were collected. The chi-square test was used for comparative analysis of relevant factors. All statistical analyses were completed by SPSS 24 software.
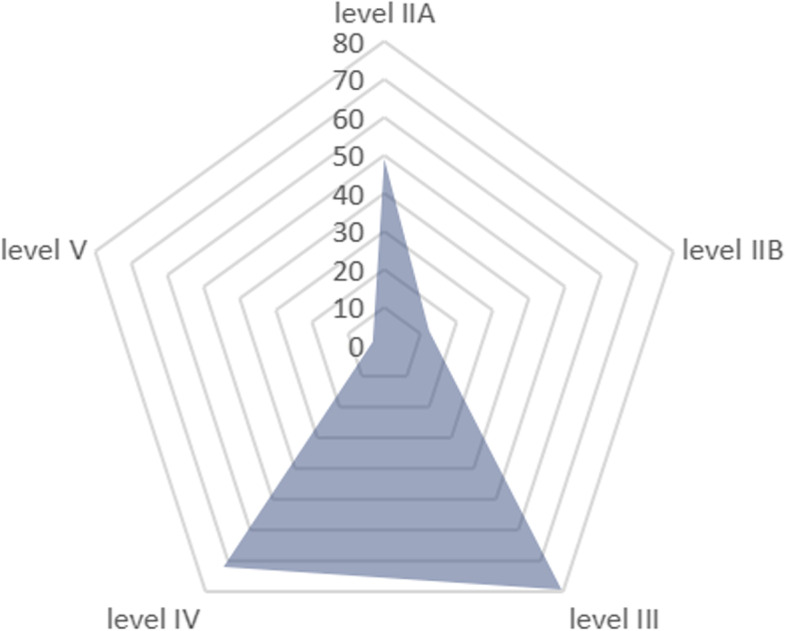
Each subgroup on sex, age, BMI, multifocality, tumor location, extrathyroidal extension, Braf gene, and lymphatic metastasis in level III, level IV, and level V had no significant difference in the positive rate of lymph node metastasis in level IIB (P > 0.05). In contrast, patients with bilateral lateral cervical lymphatic metastasis were more likely to have level IIB lymphatic metastasis than those with unilateral lateral cervical lymphatic metastasis, with a statistically significant difference (P = 0.000). In addition, lymph node metastasis in level IIA was significantly associated with lymph node metastasis in level IIB (P = 0.001). After multivariate analysis, lymph node metastasis in level IIA was independently associated with lymph node metastasis in level IIB (P = 0.010). The LCEI group had a similar lymphatic metastasis number and lymphatic metastasis rate in both level IIA and level IIB as the L-shaped incision group (P > 0.05). There were 86 patients with ipsilateral central lymphatic metastasis (78.2%). Patients with contralateral central lymphatic metastasis accounted for 56.4%. The contralateral central lymphatic metastasis rate was not correlated with age, BMI, multifocality, tumor invasion, or ipsilateral central lymphatic metastasis, and there was no significant difference (P > 0.05). The contralateral central lymphatic metastasis in males was slightly higher than that in females, and the difference was statistically significant (68.2% vs. 48.5%, P = 0.041).
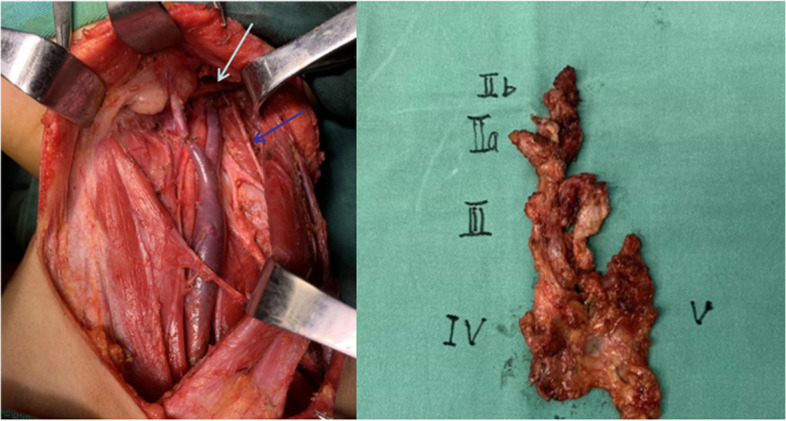
Lymphatic metastasis in level IIA was an independent predictor of lymphatic metastasis in level IIB. When bilateral lateral cervical lymphatic metastasis or lymph node metastasis of level IIA is found, lymph node dissection in level IIB is strongly recommended. When unilateral lateral cervical lymphatic metastasis and lymphatic metastasis in level IIA are negative, lymph node dissection in level IIB may be performed as appropriate on the premise of no damage to the accessory nerve. LCEI is safe and effective for lymph node dissection in level II. When the tumor is located in the unilateral lobe, attention should be given to contralateral central lymph node dissection because of the high lymphatic metastasis rate.
探讨ⅡB 区和对侧Ⅵ区淋巴结转移的相关临床因素,并评估低位颈伸切口(LCEI)在 pN1b 期甲状腺乳头状癌(PTC)行Ⅱ区淋巴结清扫术的安全性。
回顾性分析 2021 年 9 月至 2022 年 5 月在四川省肿瘤医院头颈外科治疗的 218 例 pN1b 期 PTC 患者的临床资料,收集患者年龄、性别、体质量指数(BMI)、肿瘤部位、最大肿瘤直径、多灶性、Braf 基因、T 分期、手术切口方式及各颈区淋巴结转移情况等数据,采用卡方检验进行相关因素的比较分析。所有统计学分析均使用 SPSS 24 软件完成。
在性别、年龄、BMI、多灶性、肿瘤部位、甲状腺外侵犯、Braf 基因及Ⅲ、Ⅳ、Ⅴ区淋巴结转移方面,ⅡB 区淋巴结转移阳性率在双侧颈侧区淋巴结转移和单侧颈侧区淋巴结转移亚组间差异均无统计学意义(P>0.05)。而双侧颈侧区淋巴结转移患者较单侧颈侧区淋巴结转移患者更易发生ⅡB 区淋巴结转移,差异有统计学意义(P=0.000)。此外,ⅡA 区淋巴结转移与ⅡB 区淋巴结转移显著相关(P=0.001)。多因素分析显示,ⅡA 区淋巴结转移是ⅡB 区淋巴结转移的独立危险因素(P=0.010)。LCEI 组在ⅡA 区和ⅡB 区的淋巴结转移数量和转移率与 L 形切口组相似(P>0.05)。86 例患者同侧中央区淋巴结转移(78.2%),对侧中央区淋巴结转移 56.4%。对侧中央区淋巴结转移率与年龄、BMI、多灶性、肿瘤侵袭性及同侧中央区淋巴结转移均无相关性,差异无统计学意义(P>0.05)。男性对侧中央区淋巴结转移率略高于女性,差异有统计学意义(68.2%比 48.5%,P=0.041)。
ⅡA 区淋巴结转移是ⅡB 区淋巴结转移的独立预测因子。当发现双侧颈侧区淋巴结转移或ⅡA 区淋巴结转移时,强烈建议行ⅡB 区淋巴结清扫术。当单侧颈侧区淋巴结转移和ⅡA 区淋巴结转移阴性时,在不损伤副神经的前提下,可酌情行ⅡB 区淋巴结清扫术。LCEI 用于Ⅱ区淋巴结清扫术安全有效。当肿瘤位于单侧叶时,由于其较高的淋巴结转移率,应注意对侧中央区淋巴结的清扫。