Unité de Réanimation Médicale, Service des Réanimations, Centre Hospitalier Universitaire de Nîmes, Hôpital Caremeau, Place du Prof Robert Debré, 30029, Nîmes, France.
Université de Montpellier, Montpellier, France.
Crit Care. 2023 Aug 17;27(1):316. doi: 10.1186/s13054-023-04602-7.
This substudy of the randomized IDEAL-ICU trial assessed whether the timing of renal replacement therapy (RRT) initiation has a differential effect on 90-day mortality, according to the criteria used to diagnose acute kidney injury (AKI), in patients with early-stage septic shock.
Three groups were considered according to the criterion defining AKI: creatinine elevation only (group 1), reduced urinary output only (group 2), creatinine elevation plus reduced urinary output (group 3). Primary outcome was 90-day all-cause death. Secondary endpoints were RRT-free days, RRT dependence and renal function at discharge. We assessed the interaction between RRT strategy (early vs. delayed) and group, and the association between RRT strategy and mortality in each group by logistic regression.
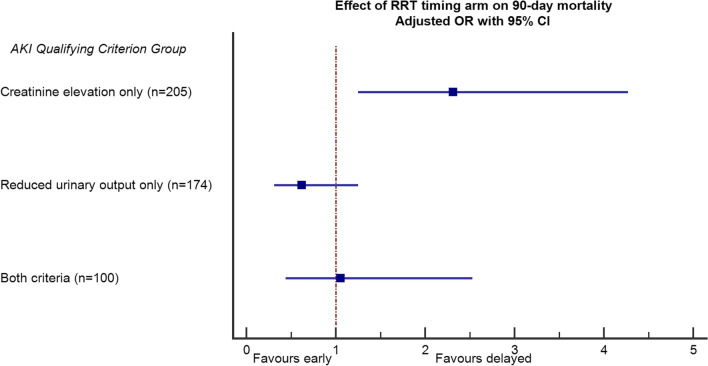
Of 488 patients enrolled, 205 (42%) patients were in group 1, 174 (35%) in group 2, and 100 (20%) in group 3. The effect of RRT initiation strategy on 90-day mortality across groups showed significant heterogeneity (adjusted interaction p = 0.021). Mortality was 58% vs. 42% for early vs. late RRT initiation, respectively, in group 1 (p = 0.028); 57% vs. 67%, respectively, in group 2 (p = 0.18); and 58% vs. 55%, respectively, in group 3 (p = 0.79). There was no significant difference in secondary outcomes.
The timing of RRT initiation has a differential impact on outcome according to AKI diagnostic criteria. In patients with elevated creatinine only, early RRT initiation was associated with significantly increased mortality. In patients with reduced urine output only, late RRT initiation was associated with a nonsignificant, 10% absolute increase in mortality.
这项 IDEAL-ICU 随机试验的亚组研究评估了在早期脓毒症休克患者中,根据急性肾损伤 (AKI) 的诊断标准,肾脏替代治疗 (RRT) 开始的时机是否对 90 天死亡率有不同影响。
根据定义 AKI 的标准,将患者分为三组:仅肌酐升高(第 1 组)、仅尿量减少(第 2 组)、肌酐升高加尿量减少(第 3 组)。主要结局为 90 天全因死亡。次要终点为无 RRT 天数、RRT 依赖和出院时肾功能。我们评估了 RRT 策略(早期与延迟)与组之间的交互作用,以及 RRT 策略与每组死亡率之间的关联,使用逻辑回归分析。
在纳入的 488 名患者中,205 名(42%)患者在第 1 组,174 名(35%)在第 2 组,100 名(20%)在第 3 组。RRT 起始策略对各组 90 天死亡率的影响存在显著异质性(调整后的交互作用 p=0.021)。第 1 组中,早期与晚期 RRT 开始的死亡率分别为 58%和 42%(p=0.028);第 2 组中,死亡率分别为 57%和 67%(p=0.18);第 3 组中,死亡率分别为 58%和 55%(p=0.79)。次要结局无显著差异。
根据 AKI 诊断标准,RRT 起始时机对预后有不同影响。仅肌酐升高的患者中,早期 RRT 起始与死亡率显著增加相关。仅尿量减少的患者中,晚期 RRT 起始与死亡率增加 10%(绝对值)相关,但无统计学意义。