Department of Rheumatology and Immunology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China.
Department of Internal Medicine, the People Hospital of Tongshan, Xianning, China.
Front Immunol. 2023 Aug 4;14:1223062. doi: 10.3389/fimmu.2023.1223062. eCollection 2023.
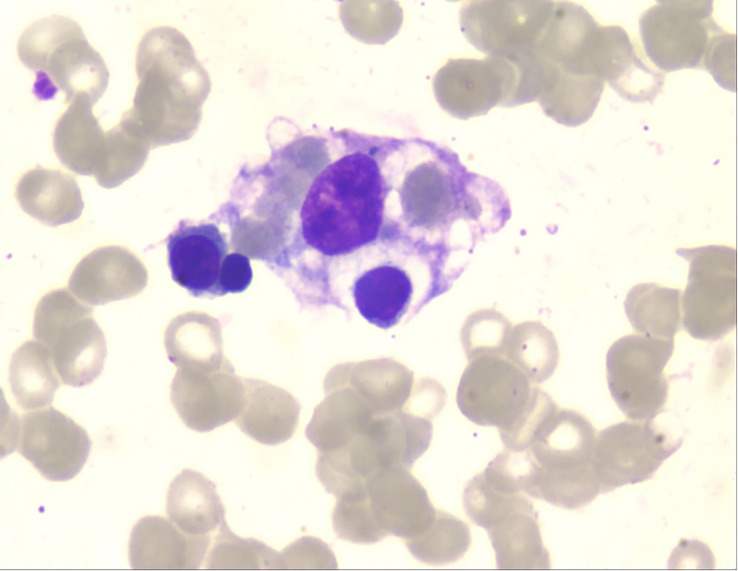
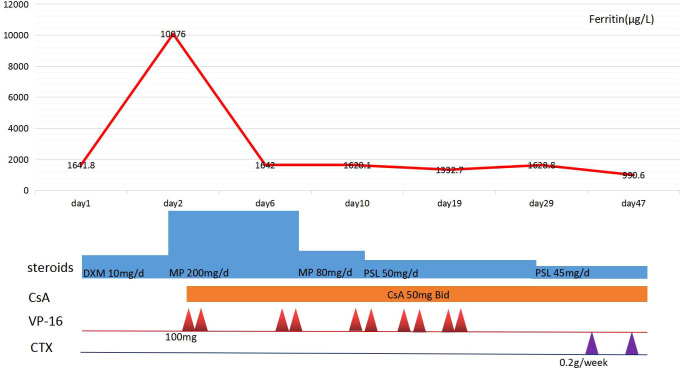
Hemophagocytic lymphohistiocytosis (HLH) is a severe and life-threatening hyperinflammatory condition characterized by excessive activation of macrophages and T cells and resulted in multi-organ dysfunction. HLH can be a primary disease or secondary to infections, malignancy, and some autoimmune diseases, including adult-onset Still's disease (AOSD) and systemic lupus erythematosus (SLE). However, it is rare for HLH to occur as a secondary condition to drug-induced lupus erythematosus (DILE). In this report, we present a case of HLH as an unusual complication during SLE treatment in a 31-year-old male patient. The patient initially suffered from active chronic hepatitis B (CHB) and was treated with pegylated INFα-2b (Peg-INFα-2b), tenofovir disoproxil and lamivudine. After 19 months, CHB obtained biochemical and virological response with HBsAg positive to HBsAb. The patient developed fever, headache, and cytopenia after Peg-INFα-2b treatment for 33 months, and laboratory studies revealed that ANA and anti dsDNA were positive. He displayed 5 features meeting the HLH-2004 criteria for diagnosis including fever, pancytopenia, hyperferritinemia, high levels of soluble CD25, and hemophagocytosis on bone marrow biopsy. The patient was initiated with a combination treatment of intravenous methylprednisolone pulse therapy, oral cyclosporine, and etoposide (VP-16), which was followed by a course of oral prednisolone, intravenous cyclophosphamide pulse therapy, and entecavir with complete response. To our knowledge, this is the first report of IFN-α induced SLE complicating with HLH. Physicians should consider the potential autoimmune side effects of IFN-α therapy and be alert to insidious HLH in patients diagnosed with SLE.
噬血细胞性淋巴组织细胞增生症(HLH)是一种严重的、危及生命的、以巨噬细胞和 T 细胞过度激活为特征的高炎症状态,导致多器官功能障碍。HLH 可以是原发性疾病,也可以继发于感染、恶性肿瘤和某些自身免疫性疾病,包括成人Still 病(AOSD)和系统性红斑狼疮(SLE)。然而,HLH 作为药物诱导的狼疮性肾炎(DILE)的继发性疾病较为罕见。在本报告中,我们介绍了一例 HLH 作为一名 31 岁男性 SLE 治疗过程中出现的不常见并发症。该患者最初患有活动性慢性乙型肝炎(CHB),接受聚乙二醇化 INFα-2b(Peg-INFα-2b)、替诺福韦酯和拉米夫定治疗。19 个月后,HBsAg 转为 HBsAb,CHB 获得生化和病毒学应答。Peg-INFα-2b 治疗 33 个月后,患者出现发热、头痛和血细胞减少,实验室研究显示 ANA 和抗 dsDNA 阳性。他表现出符合 HLH-2004 标准的 5 项特征,包括发热、全血细胞减少、高铁蛋白血症、可溶性 CD25 水平升高和骨髓活检中的噬血现象。该患者开始接受静脉注射甲基泼尼松龙脉冲治疗、口服环孢素和依托泊苷(VP-16)联合治疗,随后口服泼尼松龙、静脉注射环磷酰胺脉冲治疗和恩替卡韦治疗,获得完全缓解。据我们所知,这是首例 IFN-α 诱导的 SLE 并发 HLH 的报告。医生应考虑 IFN-α 治疗的潜在自身免疫副作用,并警惕诊断为 SLE 的患者中隐匿性 HLH 的发生。