Cuttone Giuseppe, Martucci Gennaro, Napoli Ruggero, Tigano Stefano, Arcadipane Antonio, Pappalardo Federico, Sanfilippo Filippo
Department of Anesthesia and Intensive Care, ASP Trapani, S.A. Abate Hospital, Erice, Italy.
Department of Anesthesia and Intensive Care, IRCCS-ISMETT/UPMC Italy, Palermo, Italy.
Saudi J Anaesth. 2023 Jul-Sep;17(3):394-400. doi: 10.4103/sja.sja_205_23. Epub 2023 Jun 22.
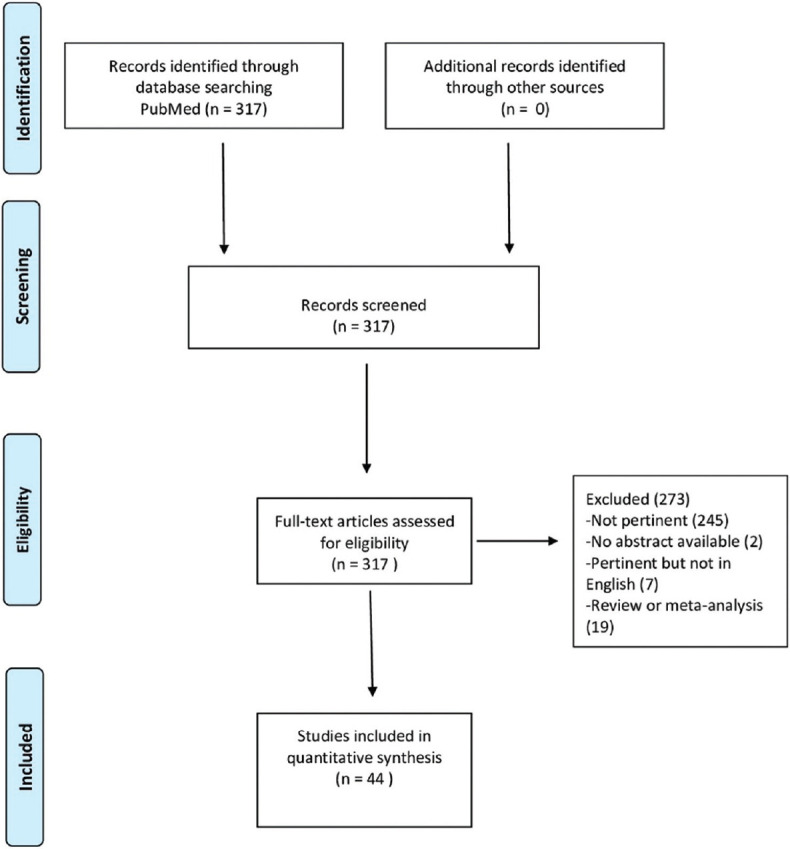
Brugada syndrome (BrS) is a major risk factor for sudden cardiac death and ventricular tachyarrhythmias. Several drugs are contraindicated in patients with BrS, including some commonly administered drugs during anesthesia or in the perioperative period; however, there is still a paucity of evidence regarding BrS and common anesthetic pharmaceuticals. We conducted a systematic literature search (PubMed, updated October 10, 2022), including all studies reporting pharmacological management of BrS patients during anesthesia or intensive care, with a specific focus on proarrhythmic effects and possible pharmacological interactions in the context of BrS. The search revealed 44 relevant items, though only three original studies. Two randomized controlled studies were identified, one comparing propofol and etomidate for the induction of general anesthesia and one investigating lidocaine with or without epinephrine for local anesthesia; there was also one prospective study without a control group. The other studies were case series (n = 5, for a total of 19 patients) or case reports (n = 36). Data are reported on a total population of 199 patients who underwent general or local anesthesia. None of the studies evaluated BrS patients in the intensive care unit (ICU). We found the studies focusing on the pharmacological management of BrS patients undergoing general or local anesthesia to be of generally poor quality. However, it appears that propofol can be used safely, without an increase in arrhythmic events. Regional anesthesia is possible, and lidocaine might be preferred over longer-acting local anesthetics. Considering the quality of the included studies and their anecdotal evidence, it seems increasingly important to conduct large multicenter studies or promote international registries with high-quality data on the anesthesiological management of these patients.
Brugada综合征(BrS)是心源性猝死和室性快速性心律失常的主要危险因素。BrS患者禁用多种药物,包括一些麻醉期间或围手术期常用药物;然而,关于BrS与常见麻醉药物的证据仍然匮乏。我们进行了系统的文献检索(PubMed,2022年10月10日更新),纳入所有报告BrS患者在麻醉或重症监护期间药物治疗的研究,特别关注BrS背景下的促心律失常作用和可能的药物相互作用。检索发现44篇相关文献,但仅有三项原创研究。确定了两项随机对照研究,一项比较丙泊酚和依托咪酯用于全身麻醉诱导,另一项研究利多卡因加或不加肾上腺素用于局部麻醉;还有一项无对照组的前瞻性研究。其他研究为病例系列(n = 5,共19例患者)或病例报告(n = 36)。报告了199例接受全身或局部麻醉患者的总体数据。没有研究评估重症监护病房(ICU)中的BrS患者。我们发现,关注BrS患者全身或局部麻醉药物治疗的研究质量普遍较差。然而,丙泊酚似乎可以安全使用,不会增加心律失常事件。区域麻醉是可行的,利多卡因可能比长效局部麻醉药更受青睐。考虑到纳入研究的质量及其轶事性证据,开展大型多中心研究或推广关于这些患者麻醉管理的高质量数据的国际注册研究似乎越来越重要。