Department of Medicine, University of Cambridge, Cambridge, UK.
Department of Internal Medicine-Nephrology, The Ohio State University, Columbus, Ohio, USA.
Lupus Sci Med. 2023 Aug;10(2). doi: 10.1136/lupus-2023-000910.
To characterise the safety and efficacy of anifrolumab in active lupus nephritis (LN) through year 2 of the phase II randomised, double-blind Treatment of Uncontrolled Lupus via the Interferon Pathway (TULIP)-LN trial (NCT02547922) of 2 anifrolumab dosing regimens versus placebo.
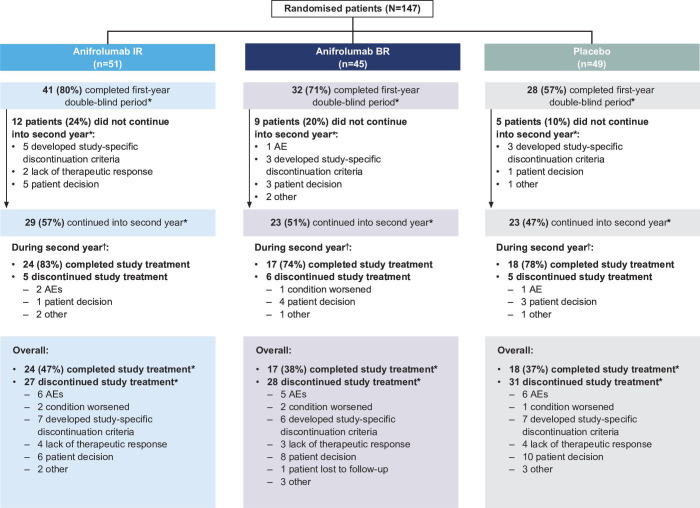
Patients received intravenous anifrolumab 900 mg for the first 3 doses followed by 300 mg anifrolumab (intensified regimen (IR)), 300 mg anifrolumab (basic regimen (BR)) or placebo every 4 weeks throughout. To continue into Year 2, patients must have achieved at least partial renal response and a glucocorticoid tapering target.
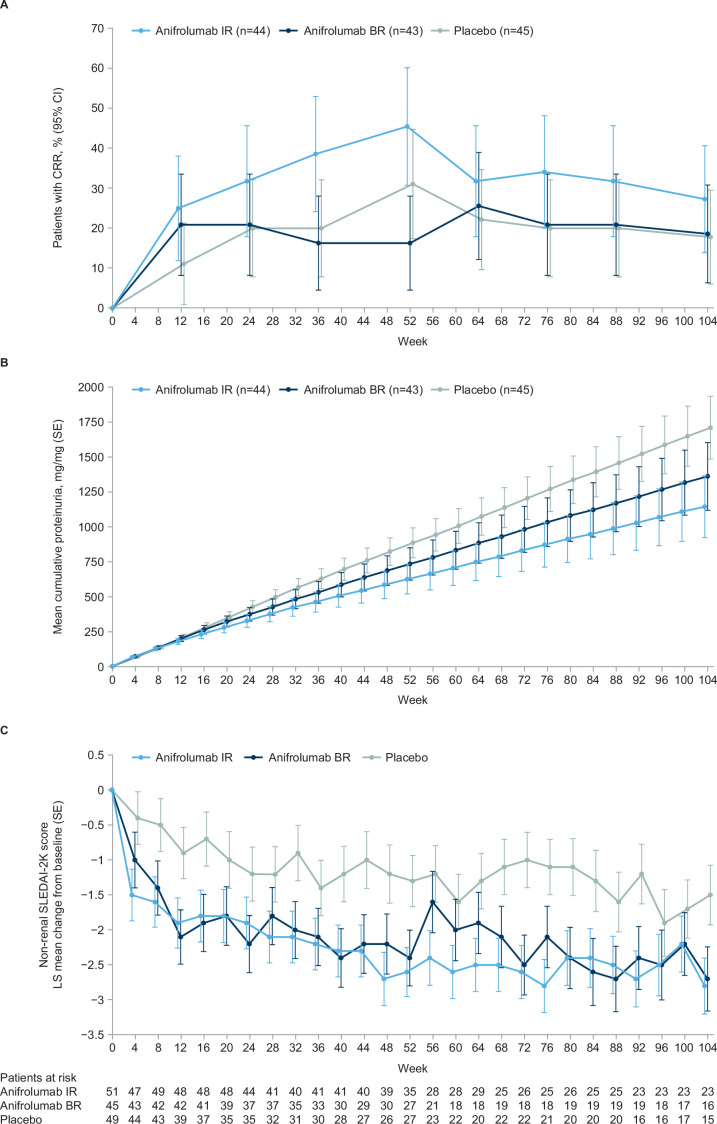
Of 147 randomised patients, 101 completed Year 1 study treatment; of these, 75 (74%) continued into Year 2 (anifrolumab IR: n=29, BR: n=23 and placebo: n=23). During Year 2, 72% of patients reported ≥1 adverse event (AE); serious AEs were reported in 6.9%, 8.7% and 8.7% of patients (anifrolumab IR, BR and placebo, respectively); 3 patients discontinued treatment due to an AE (anifrolumab IR: n=2 and placebo: n=1) and herpes zoster was reported in 2 patients (anifrolumab IR: n=1 and BR: n=1). The study was ongoing at the start of the pandemic, but no COVID-19 cases were reported. Of the 145 patients receiving treatment, more patients on the IR attained complete renal response at Week 104 compared with those on BR or placebo (27.3% vs 18.6% and 17.8%) and simultaneously achieved sustained glucocorticoid tapering (IR: 25.0%; BR: 18.6% and placebo: 17.8%). The improvements in estimated glomerular filtration rate were numerically larger in both anifrolumab groups versus placebo.
The safety and tolerability profile through Year 2 of TULIP-LN was generally consistent with Year 1, with promising efficacy results for the anifrolumab IR regimen. Collectively, the results support further investigation of an anifrolumab intensified dosing regimen in larger populations of patients with active proliferative LN.
NCT02547922.
通过治疗未控制狼疮性肾炎的干扰素通路(TULIP-LN)试验(NCT02547922)的第 2 年,评估两种不同剂量的阿尼鲁单抗治疗活动期狼疮性肾炎(LN)的安全性和疗效。该试验为随机、双盲试验,比较了阿尼鲁单抗与安慰剂治疗。
患者接受静脉注射阿尼鲁单抗 900mg,前 3 剂,随后每 4 周接受阿尼鲁单抗 300mg(强化方案(IR))、300mg(基础方案(BR))或安慰剂。要继续进入第 2 年,患者必须达到至少部分肾脏缓解和糖皮质激素减量目标。
在 147 名随机患者中,有 101 名完成了第 1 年的研究治疗;其中,75 名(74%)继续进入第 2 年(阿尼鲁单抗 IR:n=29,BR:n=23 和安慰剂:n=23)。在第 2 年期间,72%的患者报告了≥1 次不良事件(AE);阿尼鲁单抗 IR、BR 和安慰剂组分别有 6.9%、8.7%和 8.7%的患者发生严重 AE;3 名患者因 AE 停药(阿尼鲁单抗 IR:n=2,安慰剂:n=1),2 名患者报告带状疱疹(阿尼鲁单抗 IR:n=1,BR:n=1)。在大流行开始时,该研究仍在进行中,但没有报告 COVID-19 病例。在接受治疗的 145 名患者中,与 BR 或安慰剂相比,更多接受 IR 治疗的患者在第 104 周达到完全肾脏缓解(27.3% vs 18.6%和 17.8%),同时实现持续的糖皮质激素减量(IR:25.0%;BR:18.6%和安慰剂:17.8%)。与安慰剂组相比,IR 组和 BR 组的估算肾小球滤过率改善数值更大。
TULIP-LN 第 2 年的安全性和耐受性与第 1 年基本一致,IR 方案的疗效结果令人鼓舞。总的来说,这些结果支持在更大的活动性增殖性 LN 患者人群中进一步研究阿尼鲁单抗强化剂量方案。
NCT02547922。