Department of Anaesthesiology and Intensive Care, Zealand University Hospital, Lykkebækvej 1, 4600, Køge, Denmark.
Collaboration for Research in Intensive Care (CRIC), Copenhagen University Hospital - Rigshospitalet, Copenhagen, Denmark.
Crit Care. 2023 Aug 26;27(1):329. doi: 10.1186/s13054-023-04621-4.
Haloperidol is frequently used in critically ill patients with delirium, but evidence for its effects has been sparse and inconclusive. By including recent trials, we updated a systematic review assessing effects of haloperidol on mortality and serious adverse events in critically ill patients with delirium.
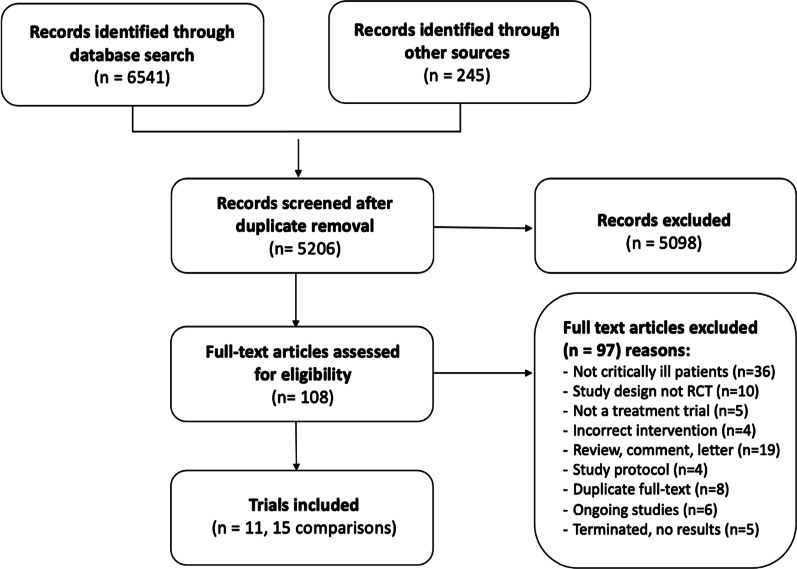
This is an updated systematic review with meta-analysis and trial sequential analysis of randomised clinical trials investigating haloperidol versus placebo or any comparator in critically ill patients with delirium. We adhered to the Cochrane handbook, the PRISMA guidelines and the grading of recommendations assessment, development and evaluation statements. The primary outcomes were all-cause mortality and proportion of patients with one or more serious adverse events or reactions (SAEs/SARs). Secondary outcomes were days alive without delirium or coma, delirium severity, cognitive function and health-related quality of life.
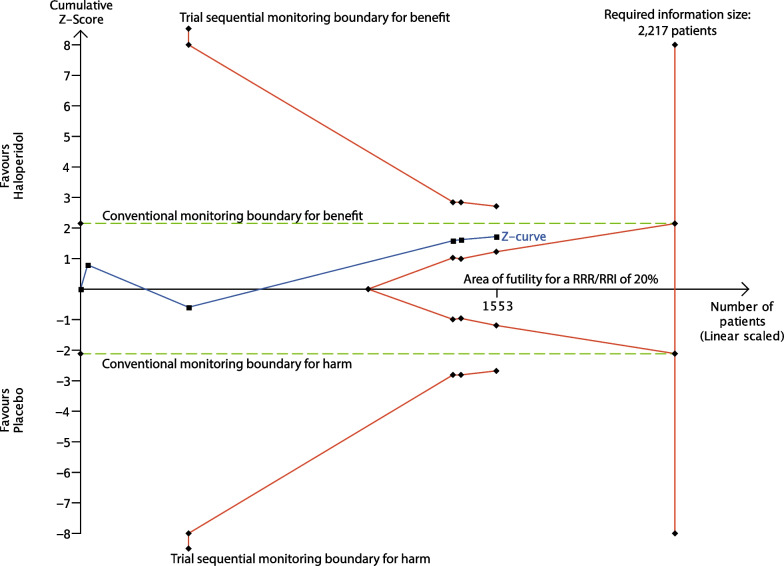
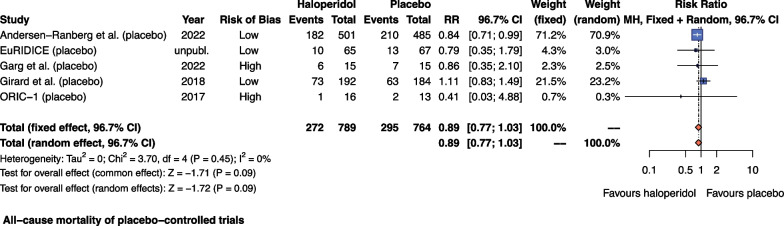
We included 11 RCTs with 15 comparisons (n = 2200); five were placebo-controlled. The relative risk for mortality with haloperidol versus placebo was 0.89; 96.7% CI 0.77 to 1.03; I = 0% (moderate-certainty evidence) and for proportion of patients experiencing SAEs/SARs 0.94; 96.7% CI 0.81 to 1.10; I = 18% (low-certainty evidence). We found no difference in days alive without delirium or coma (moderate-certainty evidence). We found sparse data for other secondary outcomes and other comparators than placebo.
Haloperidol may reduce mortality and likely result in little to no change in the occurrence of SAEs/SARs compared with placebo in critically ill patients with delirium. However, the results were not statistically significant and more trial data are needed to provide higher certainty for the effects of haloperidol in these patients.
CRD42017081133, date of registration 28 November 2017.
氟哌啶醇常用于伴有谵妄的危重症患者,但相关证据一直较为稀少且不明确。通过纳入近期的试验,我们更新了一项系统评价,评估氟哌啶醇对伴有谵妄的危重症患者死亡率和严重不良事件的影响。
这是一项更新的系统评价,采用荟萃分析和试验序贯分析,纳入了氟哌啶醇与安慰剂或任何对照药物治疗伴有谵妄的危重症患者的随机临床试验。我们遵循 Cochrane 手册、PRISMA 指南和推荐评估、制定与评价分级声明。主要结局为全因死亡率和出现 1 项或多项严重不良事件或反应(SAEs/SARs)的患者比例。次要结局为无谵妄或昏迷天数、谵妄严重程度、认知功能和健康相关生活质量。
我们纳入了 11 项 RCT,包含 15 项比较(n=2200);其中 5 项为安慰剂对照。与安慰剂相比,氟哌啶醇治疗的死亡率相对风险为 0.89;96.7% CI 0.77 至 1.03;I²=0%(中等确定性证据),SAEs/SARs 发生率的相对风险为 0.94;96.7% CI 0.81 至 1.10;I²=18%(低确定性证据)。我们发现无谵妄或昏迷天数无差异(中等确定性证据)。我们发现其他次要结局和除安慰剂以外的其他对照药物的数据稀少。
与安慰剂相比,氟哌啶醇可能降低死亡率,且可能导致伴有谵妄的危重症患者严重不良事件或反应的发生率几乎没有变化。然而,这些结果并不具有统计学意义,需要更多的试验数据来为氟哌啶醇在这些患者中的作用提供更高的确定性。
CRD42017081133,注册日期 2017 年 11 月 28 日。