Nishino Tomofumi, Hiraya Daigo, Yamamoto Yuki, Suzu Tomomi, Nishida Yusuke, Yamazaki Masashi
Department of Orthopaedic Surgery, Institute of Medicine, University of Tsukuba, Tsukuba, Ibaraki, Japan.
Department of Cardiology, Institute of Medicine, University of Tsukuba, Tsukuba, Ibaraki, Japan.
Asia Pac J Sports Med Arthrosc Rehabil Technol. 2023 Aug 21;33:1-5. doi: 10.1016/j.asmart.2023.08.005. eCollection 2023 Jul.
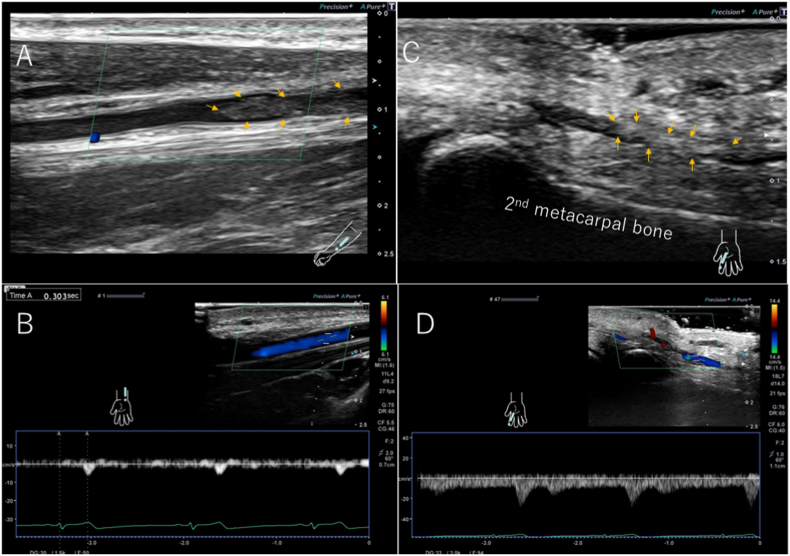
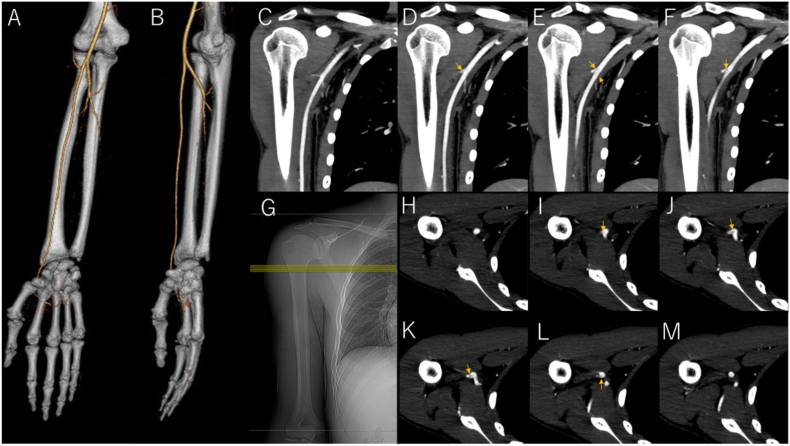
The posterior circumflex humeral artery, a branch of the axillary artery, is compressed by the humeral head during repeated abduction and external rotation of the shoulder joint owing to its anatomical structure. This damages the vascular endothelium, resulting in thrombi, arterial dissection, and aneurysms, a condition known as posterior, circumflex humeral artery pathological lesions. A thrombus may form at the site and becomes a peripheral embolus, resulting in peripheral arterial occlusion.A 21-year-old right-handed elite man college volleyball player noticed coldness and pain in his right hand during a game. Cyanosis was present except in the middle finger, and the beating radial artery was palpable; however, the ulnar artery was not. Doppler ultrasound examination revealed thrombus occlusion of the ulnar artery and common palmar artery of the index finger. Peripheral arterial occlusion was diagnosed due to embolization of a thrombus from this site. The patient stopped practicing volleyball immediately after the onset of symptoms and was started on cilostazol 200 mg and rivaroxaban 15 mg. Subjective coldness of the fingers improved one week after the start of treatment. The patient resumed practice four weeks after the start of treatment and participated in a game by the seventh week.Posterior circumflex humeral artery pathological lesions are caused by overhead motions such as pitching. They are most commonly reported in athletes playing volleyball, although rare, and many cases of aneurysm formation have been reported.Observing a cold sensation in the periphery after practice is necessary for screening.
旋肱后动脉是腋动脉的一个分支,由于其解剖结构,在肩关节反复外展和外旋过程中会受到肱骨头的压迫。这会损伤血管内皮,导致血栓形成、动脉夹层和动脉瘤,这种情况被称为旋肱后动脉病理性病变。血栓可能在该部位形成并成为周围栓子,导致周围动脉闭塞。一名21岁的右利手精英男子大学排球运动员在比赛中注意到右手发冷和疼痛。除中指外,手部出现发绀,桡动脉搏动可触及,但尺动脉未触及。多普勒超声检查显示尺动脉和食指掌总动脉血栓闭塞。诊断为该部位血栓栓塞导致的周围动脉闭塞。患者症状出现后立即停止排球训练,并开始服用西洛他唑200毫克和利伐沙班15毫克。治疗开始一周后,手指主观发冷症状有所改善。治疗开始四周后患者恢复训练,到第七周时参加了一场比赛。旋肱后动脉病理性病变是由投球等过头动作引起的。虽然罕见,但在排球运动员中报道最多,并且已经报道了许多动脉瘤形成的病例。训练后观察外周是否有冷感对于筛查很有必要。