Rodriguez-Quintero Jorge Humberto, Kamel Mohamed K, Dawodu Gbalekan, Elbahrawy Mostafa, Vimolratana Marc, Chudgar Neel P, Stiles Brendon M
Department of Cardiovascular and Thoracic Surgery, Montefiore Medical Center/Albert Einstein College of Medicine, Bronx, New York.
Department of Cardiothoracic Surgery, University of Rochester Medical Center, Rochester, New York.
JTO Clin Res Rep. 2023 Jun 30;4(8):100547. doi: 10.1016/j.jtocrr.2023.100547. eCollection 2023 Aug.
Recent trials have reported promising results with the addition of immunotherapy to chemotherapy for patients with locally advanced NSCLC, but in practice, the proportion of patients who receive systemic therapy (ST) has historically been low. Underutilization of ST may be particularly apparent in patients undergoing pneumonectomy, in whom the physiologic insult and surgical complications may preclude adjuvant therapy (ADJ). We, therefore, evaluated the use of ST for patients with NSCLC undergoing pneumonectomy.
We queried the National Cancer Database, including all patients with NSCLC who underwent pneumonectomy between 2006 and 2018. Logistic regression was used to identify associations with ST and neo-ADJ (NEO). Overall survival was compared after propensity score matching (1:1) patients undergoing ST to those undergoing surgery alone using Kaplan-Meier and Cox regression methods.
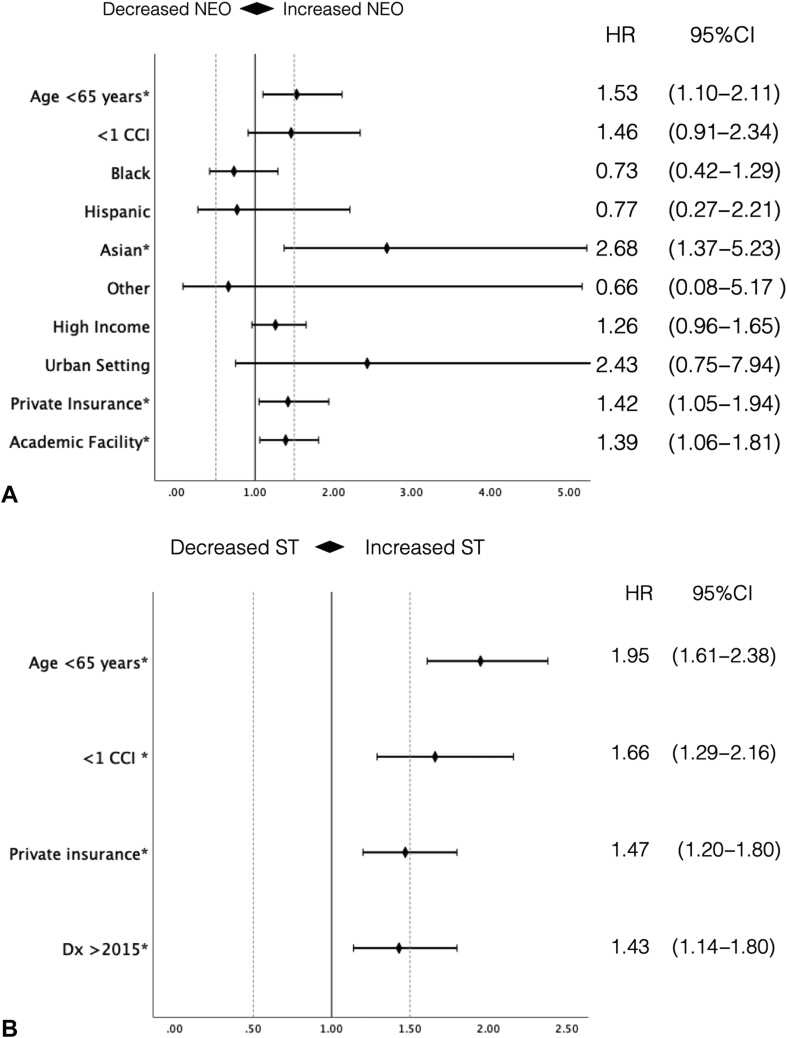
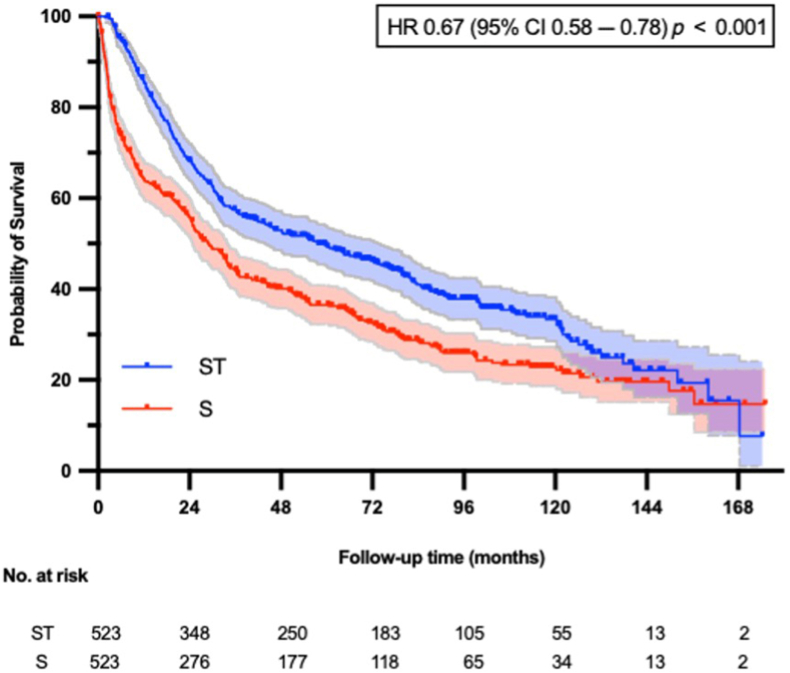
A total of 2619 patients were identified. Among these, 12% received NEO, 43% received ADJ, and 45% surgery alone. Age younger than 65 years (adjusted odds ratio [aOR] = 1.53, 95% confidence interval; [CI]: 1.10-2.11), Asian ethnicity (aOR = 2.68, 95% CI: 1.37-5.23), treatment at a high-volume center (aOR = 1.39, 95% CI: 1.06-1.81), and private insurance (aOR = 1.42, 95% CI: 1.05-1.94) were associated with NEO, whereas age younger than 65 years (aOR = 1.95, 95% CI: 1.61-2.38), comorbidity index less than or equal to 1 (aOR = 1.66, 95% CI: 1.29-2.16), and private insurance (aOR = 1.47, 95% CI: 1.20-1.80) were associated with any ST. In the matched cohort, ST was associated with better survival than surgery (adjusted hazard ratio = 0.67, 95% CI: 0.58-0.78).
A high proportion of patients who undergo pneumonectomy do not receive ST. Patient and socioeconomic factors are associated with the receipt of ST. Given its survival benefit, emphasis should be placed on multimodal treatment strategies, perhaps with greater consideration given to neoadjuvant approaches.
近期试验报告称,对于局部晚期非小细胞肺癌(NSCLC)患者,在化疗基础上加用免疫疗法取得了令人鼓舞的结果,但在实际应用中,接受全身治疗(ST)的患者比例历来较低。ST利用不足在接受肺切除术的患者中可能尤为明显,因为这些患者的生理损伤和手术并发症可能会妨碍辅助治疗(ADJ)。因此,我们评估了接受肺切除术的NSCLC患者使用ST的情况。
我们查询了国家癌症数据库,纳入了2006年至2018年间所有接受肺切除术的NSCLC患者。采用逻辑回归分析来确定与ST和新辅助治疗(NEO)相关的因素。使用倾向评分匹配(1:1)方法将接受ST的患者与仅接受手术的患者进行匹配后,采用Kaplan-Meier法和Cox回归法比较总生存期。
共识别出2619例患者。其中,12%接受了NEO,43%接受了ADJ,45%仅接受了手术。年龄小于65岁(调整比值比[aOR]=1.53,95%置信区间[CI]:1.10-2.11)、亚裔种族(aOR=2.68,95%CI:1.37-5.23)、在高容量中心接受治疗(aOR=1.39,95%CI:1.06-1.81)以及拥有私人保险(aOR=1.42,95%CI:1.05-1.94)与NEO相关,而年龄小于65岁(aOR=1.95,95%CI:1.61-2.38)、合并症指数小于或等于1(aOR=1.66,95%CI:1.29-2.16)以及拥有私人保险(aOR=1.47,95%CI:1.20-1.80)与任何ST相关。在匹配队列中,ST与比手术更好的生存相关(调整风险比=0.67,95%CI:0.58-0.78)。
接受肺切除术的患者中很大一部分未接受ST。患者和社会经济因素与接受ST相关。鉴于其生存获益,应强调多模式治疗策略,或许应更多地考虑新辅助治疗方法。