Department of Cardiothoracic and Vascular Surgery, Montefiore Medical Center/Albert Einstein College of Medicine, Bronx, NY, USA.
Division of Thoracic and Foregut Surgery, University of Rochester Medical Center, Rochester, NY, USA.
Eur J Cardiothorac Surg. 2024 Mar 1;65(3). doi: 10.1093/ejcts/ezae009.
Recent randomized data support the perioperative benefits of minimally invasive surgery (MIS) for non-small-cell lung cancer (NSCLC). Its utility for cT4 tumours remains understudied. We, therefore, sought to analyse national trends and outcomes of minimally invasive resections for cT4 cancers.
Using the 2010-2019 National Cancer Database, we identified patients with cT4N0-1 NSCLC. Patients were stratified by surgical approach. Multivariable logistic analysis was used to identify factors associated with use of a minimally invasive approach. Groups were matched using propensity score analysis to evaluate perioperative and survival end points.
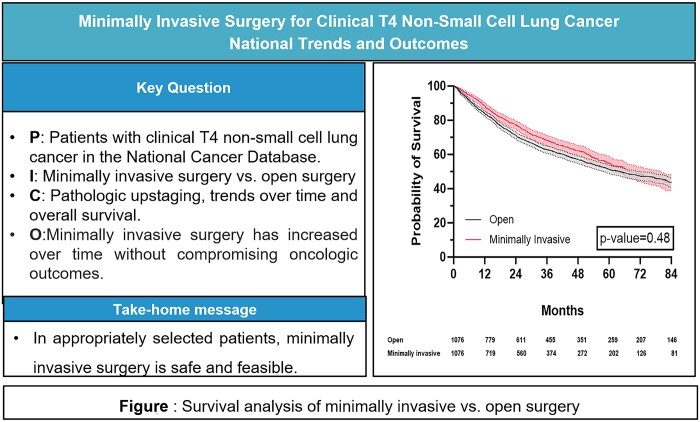
The study identified 3715 patients, among whom 64.1% (n = 2381) underwent open resection and 35.9% (n = 1334) minimally invasive resection [robotic-assisted in 31.5% (n = 420); and video-assisted in 68.5% (n = 914)]. Increased MIS use was noted among patients with higher income [≥$40 227, odds ratio (OR) 1.24; 95% confidence interval (CI) 1.01-1.51] and those treated at academic hospitals (OR 1.25; 95% CI 1.07-1.45). Clinically node-positive patients (OR 0.68; 95% CI 0.55-0.83) and those who underwent neoadjuvant therapy (OR 0.78; 95% CI 0.65-0.93) were less likely to have minimally invasive resection. In matched groups, patients undergoing MIS had a shorter median length of stay (5 vs 6 days, P < 0.001) and no significant differences between 30-day readmissions or 30/90-day mortality. MIS did not compromise overall survival (log-rank P = 0.487).
Nationally, the use of minimally invasive approaches for patients with cT4N0-1M0 NSCLC has increased substantially. In these patients, MIS is safe and does not compromise perioperative outcomes or survival.
最近的随机数据支持微创外科(MIS)在非小细胞肺癌(NSCLC)中的围手术期获益。其在 cT4 肿瘤中的应用仍研究不足。因此,我们试图分析 cT4 癌症微创切除术的全国趋势和结果。
我们使用 2010-2019 年国家癌症数据库,确定了 cT4N0-1 NSCLC 患者。患者按手术方式分层。多变量逻辑分析用于确定与微创方法使用相关的因素。通过倾向评分分析对各组进行匹配,以评估围手术期和生存终点。
该研究共纳入 3715 例患者,其中 64.1%(n=2381)接受了开放性切除术,35.9%(n=1334)接受了微创切除术[机器人辅助手术 31.5%(n=420);视频辅助手术 68.5%(n=914)]。较高的收入(≥$40227)和在学术医院治疗的患者中,MIS 的使用有所增加(优势比 [OR] 1.24;95%置信区间 [CI] 1.01-1.51)。临床淋巴结阳性患者(OR 0.68;95%CI 0.55-0.83)和接受新辅助治疗的患者(OR 0.78;95%CI 0.65-0.93)不太可能接受微创切除术。在匹配组中,接受 MIS 的患者的中位住院时间更短(5 天与 6 天,P<0.001),30 天再入院率或 30/90 天死亡率无显著差异。MIS 并未影响总体生存率(对数秩检验 P=0.487)。
在全国范围内,cT4N0-1M0 NSCLC 患者微创方法的使用大幅增加。在这些患者中,MIS 是安全的,不会影响围手术期结局或生存率。