Department of Internal Medicine II, Hematology, Oncology, Clinical Immunology and Rheumatology, University Hospital Tübingen, Tübingen.
University Medical Center Freiburg, Department of Hematology, Oncology and Stem Cell Transplantation, Faculty of Medicine, University of Freiburg, Freiburg.
Haematologica. 2024 Feb 1;109(2):431-443. doi: 10.3324/haematol.2023.283175.
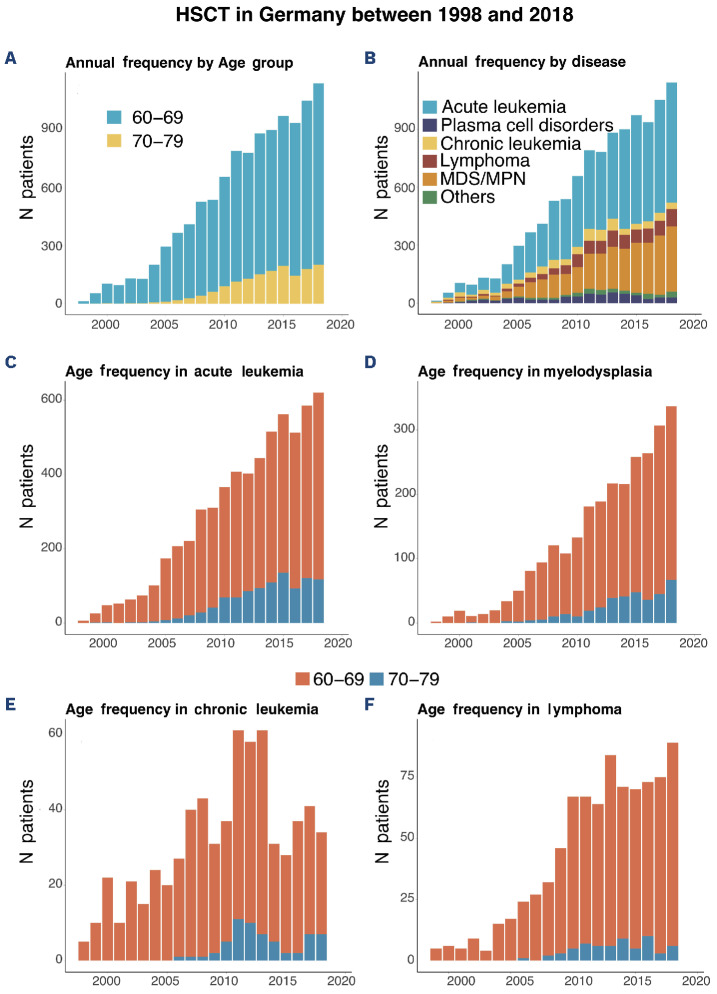
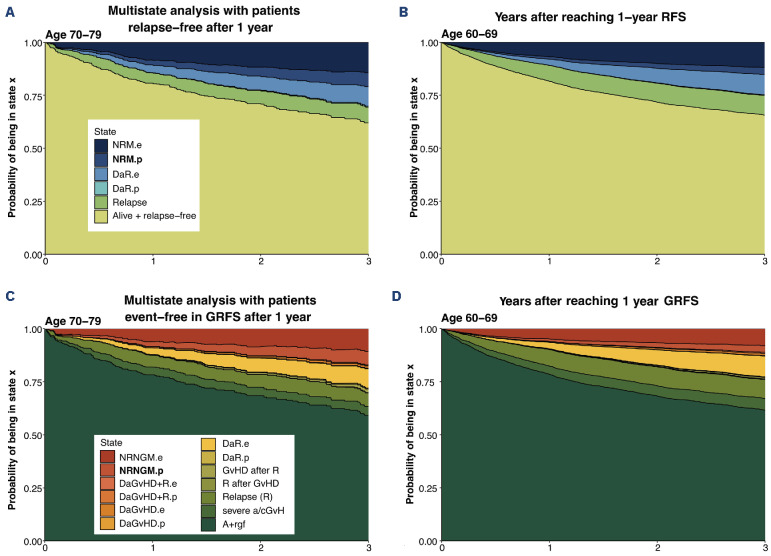
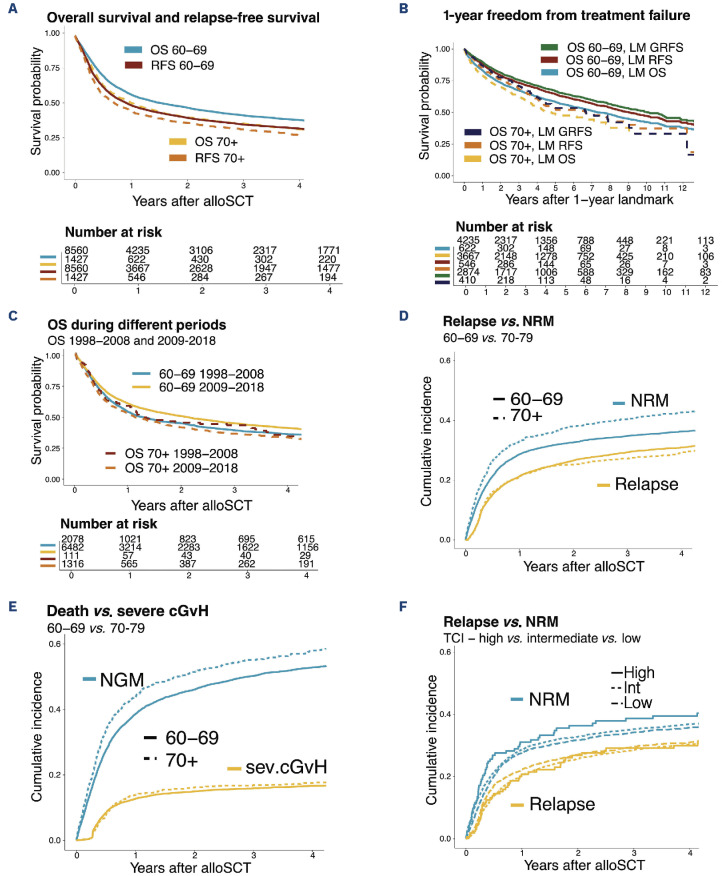
Incidences of diseases treated with transplantation frequently peak at higher age. The contribution of age to total risk of transplantation has not been estimated amidst an aging society. We compare outcomes of 1,547 patients aged 70-79 years and 9,422 patients aged 60-69 years transplanted 1998-2018 for myeloid, lymphoid and further neoplasia in Germany. To quantify the contribution of population mortality to survival, we derive excess mortality based on a sex-, year- and agematched German population in a multistate model that incorporates relapse and graft-versus-host-disease (GvHD). Overall survival, relapse-free survival (RFS) and GvHD-free-relapse-free survival (GRFS) is inferior in patients aged 70-79 years, compared to patients aged 60-69 years, with 36% (95% Confidence Interval [CI]: 34-39%) versus 43% (41-44%), 32% (30- 35%) versus 36% (35-37%) and 23% (21-26%) versus 27% (26-28%) three years post-transplant (P<0.001). Cumulative incidences of relapse at three years are 27% (25-30%) for patients aged 70-79 versus 29% (29-30%) (60-69 years) (P=0.71), yet the difference in non-relapse mortality (NRM) (40% [38-43%] vs. 35% [34-36%] in patients aged 70-79 vs. 60-69 years) (P<0.001) translates into survival differences. Median OS of patients surviving >1 year relapse-free is 6.7 (median, 95% CI: 4.5-9.4, 70-79 years) versus 9 (8.4-10.1, 60-69 years) years since landmark. Three years after RFS of one year, excess NRM is 14% (95% CI: 12-18%) in patients aged 70-79 versus 12% [11-13%] in patients aged 60-69, while population NRM is 7% (6-7%) versus 3% (3-3%). Mortality for reasons other than relapse, GvHD, or age is as high as 27% (24-29%) and 22% (22-23%) four years after transplantation. In conclusion, survival amongst older patients is adequate after allogeneic stem cell transplantation.
在接受移植治疗的疾病中,发病率经常在较高年龄达到峰值。在老龄化社会中,尚未评估年龄对移植总风险的贡献。我们比较了 1998 年至 2018 年间在德国接受同种异体骨髓、淋巴和其他肿瘤移植的 70-79 岁和 60-69 岁的 1547 例患者和 9422 例患者的结局。为了量化人群死亡率对生存率的影响,我们根据性别、年份和年龄匹配的德国人群,在包含复发和移植物抗宿主病(GvHD)的多状态模型中得出超额死亡率。与 60-69 岁的患者相比,70-79 岁的患者的总生存率、无复发存活率(RFS)和无 GvHD-无复发存活率(GRFS)较差,分别为 36%(95%置信区间[CI]:34-39%)和 43%(41-44%)、32%(30-35%)和 36%(35-37%)和 23%(21-26%)和 27%(26-28%)(P<0.001)。移植后三年的复发累积发生率为 27%(25-30%)(70-79 岁)和 29%(29-30%)(60-69 岁)(P=0.71),但非复发死亡率(NRM)的差异(40%[38-43%]与 35%[34-36%],70-79 岁与 60-69 岁)(P<0.001)导致生存差异。无复发存活>1 年的患者的中位 OS 为 6.7(中位数,95%CI:4.5-9.4,70-79 岁)和 9(8.4-10.1,60-69 岁)年(自里程碑起)。在 RFS 为一年的三年后,70-79 岁患者的超额 NRM 为 14%(95%CI:12-18%),而 60-69 岁患者为 12%[11-13%],而人群 NRM 为 7%(6-7%)和 3%(3-3%)。除复发、GvHD 或年龄以外的其他原因导致的死亡率高达 27%(24-29%)和 22%(22-23%),在移植后四年。总之,在接受异基因造血干细胞移植后,老年患者的生存情况尚可。