Canadian Medical Protective Association, Department of Safe Medical Care, Ottawa, ON, Canada.
Faculty of Medicine, Department of Emergency Medicine, University of Ottawa, Ottawa, ON, Canada.
CJEM. 2023 Sep;25(9):768-775. doi: 10.1007/s43678-023-00576-1. Epub 2023 Aug 30.
Physician documentation plays a central role in the delivery of safe patient care. It describes a physician's clinical decision-making and supports essential communication between healthcare providers within the patient's circle of care. Good documentation can potentially also decrease a physician's medico-legal risk. This study provides examples of documentation issues attributed to physicians practicing emergency medicine as identified by peer experts in civil legal actions, regulatory authority complaints (College) and hospital complaints (collectively, medico-legal cases) in Canada.
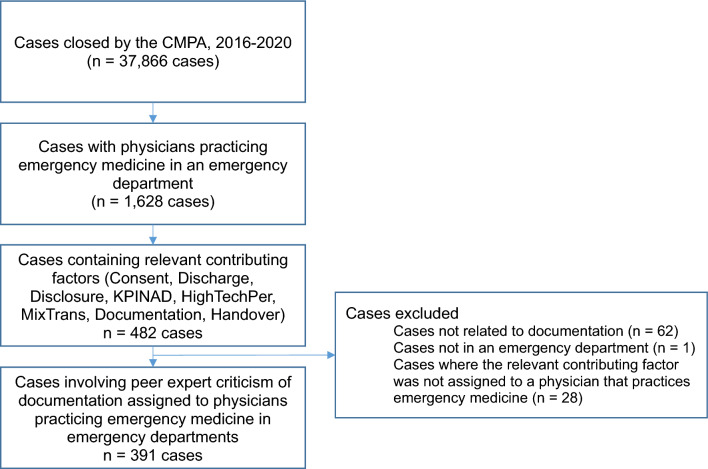
We conducted a descriptive study and content analysis of medico-legal cases involving emergency department physicians from a national repository at the Canadian Medical Protective Association. Cases with peer expert criticism of an emergency physician's documentation, which were closed between 2016 and 2020, and occurred in an emergency department were included in our analysis.
Of the 1628 cases involving emergency medicine, our inclusion criteria identified that absent or insufficiently detailed documentation was present in 24% of cases (391/1,628). A detailed review of 20% of the cases (79/391), selected randomly, found that documentation issues were most often associated with the assessment and investigation stage of care. This pertained to documenting details of the clinical examination, relevant medical history, diagnosis, and differential diagnosis.
For physicians practicing emergency medicine, criticism of documentation was frequently observed in medico-legal cases. Based on the findings of this study and the expert criticism related to documentation, emergency medicine physicians may consider reflecting upon their documentation of the care provided to determine if their documentation provides a clear and accurate chronicle of the care and the rationale for their clinical decisions.
医生的记录在提供安全的患者护理中起着核心作用。它描述了医生的临床决策,并支持患者护理圈中医疗保健提供者之间的重要沟通。良好的记录还有可能降低医生的法律风险。本研究提供了加拿大民事法律诉讼、监管机构投诉(学院)和医院投诉(统称医疗法律案件)中同行专家认定的急诊医生记录问题的示例。
我们对加拿大医疗保护协会国家档案库中涉及急诊医生的医疗法律案件进行了描述性研究和内容分析。我们的分析包括 2016 年至 2020 年期间解决的、同行专家对急诊医生记录提出批评且发生在急诊室的案例。
在涉及急诊医学的 1628 例病例中,我们的纳入标准确定,391/1628 例(24%)的病例存在或记录不充分。对随机抽取的 20%(79/391)的病例进行详细审查发现,记录问题最常与护理评估和调查阶段有关。这涉及记录临床检查、相关病史、诊断和鉴别诊断的详细信息。
对于从事急诊医学的医生来说,记录问题在医疗法律案件中经常受到批评。基于这项研究的发现以及与记录相关的专家批评,急诊医生可能会考虑反思他们提供的护理记录,以确定他们的记录是否清晰准确地记录了护理过程和临床决策的理由。