Department of Medicine, Women's College Hospital, Room 6452, 76 Grenville Street, Toronto, ON M5S 1B2, Canada.
Department of Medicine, University Health Network, 200 Elizabeth Street, Toronto, ON M5G 2C4, Canada.
Eur Heart J. 2024 Jan 7;45(2):104-113. doi: 10.1093/eurheartj/ehad508.
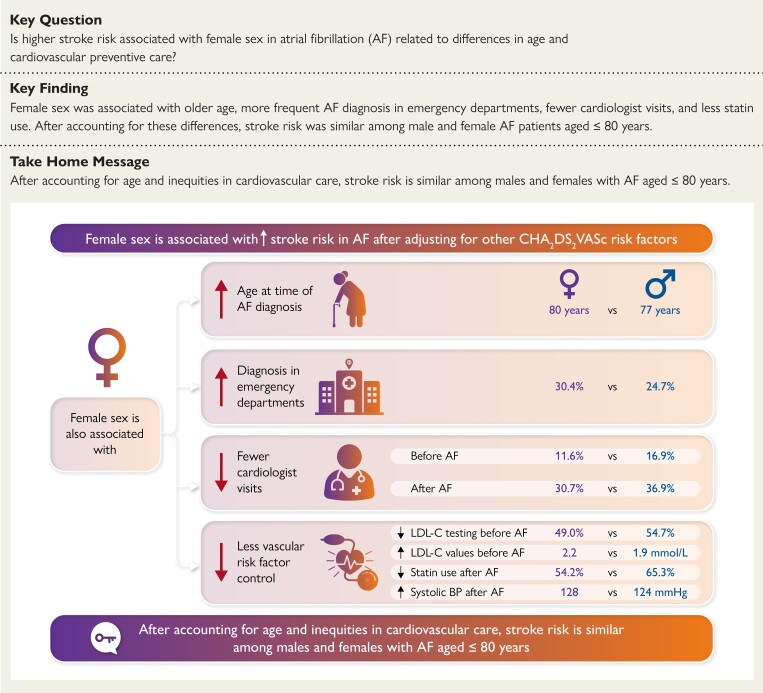
Female sex is associated with higher rates of stroke in atrial fibrillation (AF) after adjustment for other CHA2DS2-VASc factors. This study aimed to describe sex differences in age and cardiovascular care to examine their relationship with stroke hazard in AF.
Population-based cohort study using administrative datasets of people aged ≥66 years diagnosed with AF in Ontario between 2007 and 2019. Cause-specific hazard regression was used to estimate the adjusted hazard ratio (HR) for stroke associated with female sex over a 2-year follow-up. Model 1 included CHA2DS2-VASc factors, with age modelled as 66-74 vs. ≥ 75 years. Model 2 treated age as a continuous variable and included an age-sex interaction term. Model 3 further accounted for multimorbidity and markers of cardiovascular care.
The cohort consisted of 354 254 individuals with AF (median age 78 years, 49.2% female). Females were more likely to be diagnosed in emergency departments and less likely to receive cardiologist assessments, statins, or LDL-C testing, with higher LDL-C levels among females than males. In Model 1, the adjusted HR for stroke associated with female sex was 1.27 (95% confidence interval 1.21-1.32). Model 2 revealed a significant age-sex interaction, such that female sex was only associated with increased stroke hazard at age >70 years. Adjusting for markers of cardiovascular care and multimorbidity further decreased the HR, so that female sex was not associated with increased stroke hazard at age ≤80 years.
Older age and inequities in cardiovascular care may partly explain higher stroke rates in females with AF.
在调整 CHA2DS2-VASc 因素后,女性在房颤(AF)中发生中风的比率更高。本研究旨在描述 AF 中年龄和心血管护理方面的性别差异,以检查其与中风风险的关系。
本研究为基于人群的队列研究,使用安大略省 2007 年至 2019 年间诊断为 AF 的年龄≥66 岁人群的行政数据集。使用特定病因的风险回归来估计 2 年随访期间女性性别与中风相关的调整后的风险比(HR)。模型 1 包括 CHA2DS2-VASc 因素,将年龄建模为 66-74 岁与≥75 岁。模型 2 将年龄视为连续变量,并纳入年龄-性别交互项。模型 3 进一步考虑了多种合并症和心血管护理标志物。
该队列包括 354254 名患有 AF 的患者(中位数年龄为 78 岁,49.2%为女性)。女性更有可能在急诊科就诊,而不太可能接受心脏病专家评估、他汀类药物或 LDL-C 检测,女性的 LDL-C 水平高于男性。在模型 1 中,与女性性别相关的中风调整后 HR 为 1.27(95%置信区间 1.21-1.32)。模型 2 显示出显著的年龄-性别交互作用,即只有在年龄>70 岁时,女性性别才与中风风险增加相关。进一步调整心血管护理和多种合并症标志物会进一步降低 HR,因此在年龄≤80 岁时,女性性别与中风风险增加无关。
年龄较大和心血管护理方面的不平等可能部分解释了 AF 中女性中风发生率较高的原因。