Division of Hematology, Department of Medicine, University of Colorado Anschutz Medical Campus, Aurora, CO.
Division of Hematology and Medical Oncology, Weill Cornell Medicine, New York-Presbyterian, New York City, NY.
Blood Adv. 2023 Nov 14;7(21):6430-6440. doi: 10.1182/bloodadvances.2023010162.
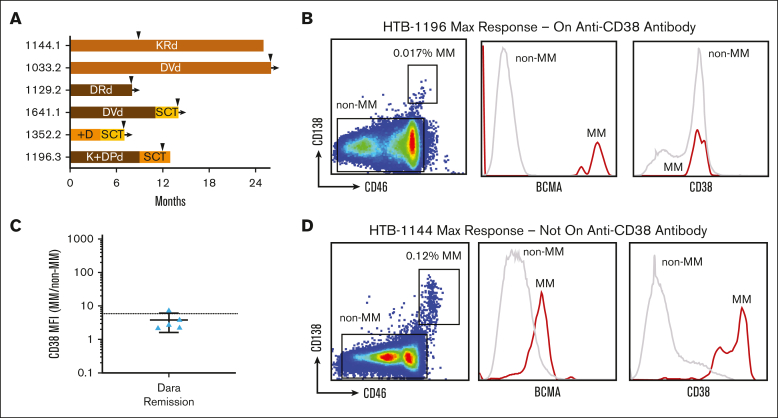
Monoclonal antibodies targeting CD38 are important for treatment of both newly diagnosed and relapsed multiple myeloma (MM). Daratumumab and isatuximab are anti-CD38 antibodies with the US Food and Drugs Administration approval in multiple different combinations. Despite good initial efficacy, patients inevitably develop drug resistance. Whether patients can be effectively re-treated with these antibodies in subsequent lines of therapy is unclear. Thus far, studies have mostly been limited to clinical retrospectives with short washout periods. To answer whether patients regain sensitivity after longer washouts, we used ex vivo sensitivity testing to isolate the anti-CD38 antibody-specific cytotoxicity in samples obtained from patients who had been exposed to and then off daratumumab for up to 53 months. MM cells from patients who had been off daratumumab for >1 year showed greater sensitivity than those with <1 year, although they still were less sensitive than those who were daratumumab naïve. CD38 expression on MM cells gradually recovered, although, again, not to the level of anti-CD38 antibody-naïve patients. Interestingly, low MM CD38 explained only 45% of cases identified to have daratumumab resistance. With clinical follow-up, we found ex vivo sensitivity predicted subsequent clinical response but CD38 overexpression did not. Patients clinically re-treated with anti-CD38 antibodies had <6 months of clinical benefit, but 1 patient who was daratumumab exposed but not refractory achieved complete response lasting 13 months. We conclude that transient efficacy can be achieved by waiting 1 year before CD38 antibody rechallenge, but this approach may be best used as a bridge to, or after, chimeric antigen receptor T-cell therapy.
针对 CD38 的单克隆抗体对新诊断和复发多发性骨髓瘤(MM)的治疗都很重要。达雷妥尤单抗和伊沙妥昔单抗是两种抗 CD38 抗体,已获得美国食品和药物管理局(FDA)在多种不同组合中的批准。尽管初始疗效良好,但患者不可避免地会产生耐药性。在后续治疗线中,这些抗体是否能有效地重新治疗患者尚不清楚。迄今为止,这些研究主要局限于具有较短洗脱期的临床回顾性研究。为了回答患者在更长的洗脱期后是否能恢复敏感性,我们使用体外敏感性测试来分离从已接受达雷妥尤单抗治疗并停药长达 53 个月的患者样本中获得的抗 CD38 抗体特异性细胞毒性。与停药时间<1 年的患者相比,停药时间>1 年的患者的 MM 细胞对达雷妥尤单抗的敏感性更高,尽管它们仍然不如初次使用达雷妥尤单抗的患者敏感。尽管 MM 细胞上的 CD38 表达逐渐恢复,但仍未恢复到抗 CD38 抗体初治患者的水平。有趣的是,MM CD38 低表达仅能解释 45%的被鉴定为达雷妥尤单抗耐药的病例。随着临床随访,我们发现体外敏感性预测了随后的临床反应,但 CD38 过表达没有预测作用。临床重新接受抗 CD38 抗体治疗的患者获益<6 个月,但有 1 名达雷妥尤单抗暴露但无耐药的患者获得了持续 13 个月的完全缓解。我们得出结论,在 CD38 抗体再次挑战前等待 1 年可以获得短暂的疗效,但这种方法最好用作嵌合抗原受体 T 细胞治疗的桥梁或之后的治疗方法。