Diwan Vishal, Hoy Wendy E, Wang Zaimin, Zhang Jianzhen, Cameron Anne, Venuthurupalli Sree K, Fassett Robert G, Chan Samuel, Healy Helen G, Tan Ken-Soon, Baer Richard, Mallett Andrew J, Gray Nicholas, Mantha Murty, Cherian Roy, Mutatiri Clyson, Madhan Krishan, Kan George, Mitchell Geoffrey, Hossain Shahadat, Wu Danielle, Han Thin, Kark Adrian, Titus Thomas, Ranganathan Dwarakanatan, Bonner Ann, Govindarajulu Sridevi
NHMRC CKD.CRE and CKD.QLD, Brisbane, Queensland, Australia.
Faculty of Medicine, The University of Queensland, Brisbane, Queensland, Australia.
Kidney Med. 2023 Jul 26;5(9):100700. doi: 10.1016/j.xkme.2023.100700. eCollection 2023 Sep.
RATIONALE & OBJECTIVE: Little is known about hospital admissions in nondialysis patients with chronic kidney disease (CKD) before death or starting kidney replacement therapy (KRT).
Retrospective observational cohort study.
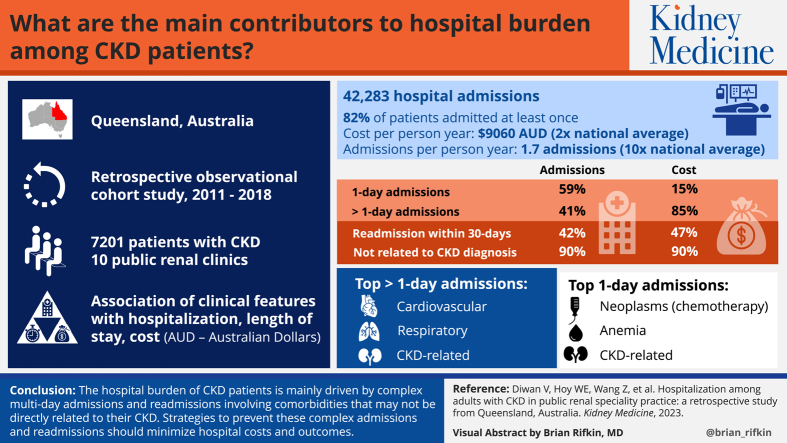
SETTING & PARTICIPANTS: Hospitalizations among 7,201 patients with CKD from 10 public renal clinics in Queensland (QLD), enrolled in the CKD.QLD registry starting in May 2011, were followed for 25,496.34 person-years until they started receiving KRT or died, or until June 30, 2018.
Demographic and clinical characteristics of patients with CKD.
Hospital admissions.
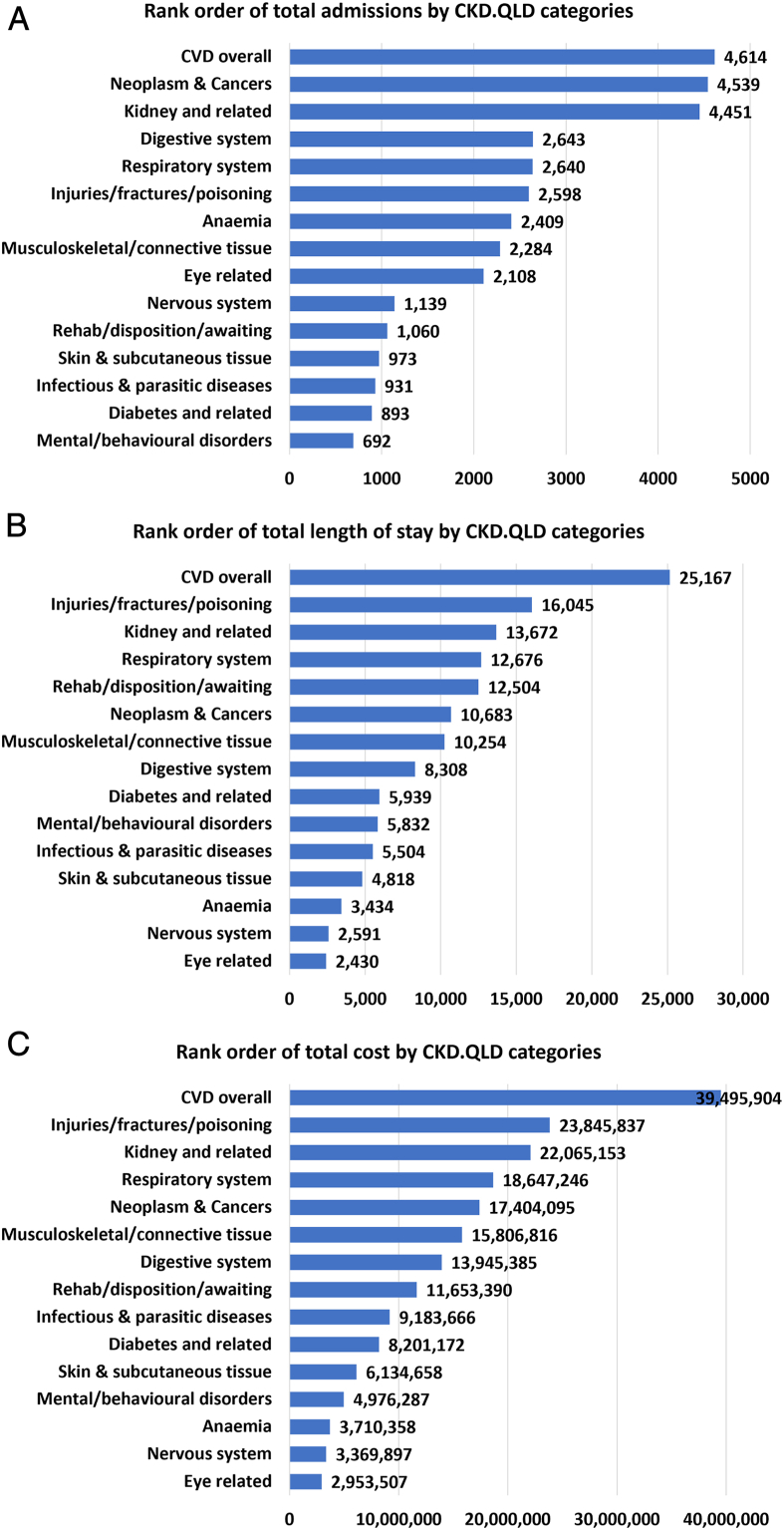
We evaluated the association of demographic and clinical features with hospitalizations, length of hospital stay, and cost.
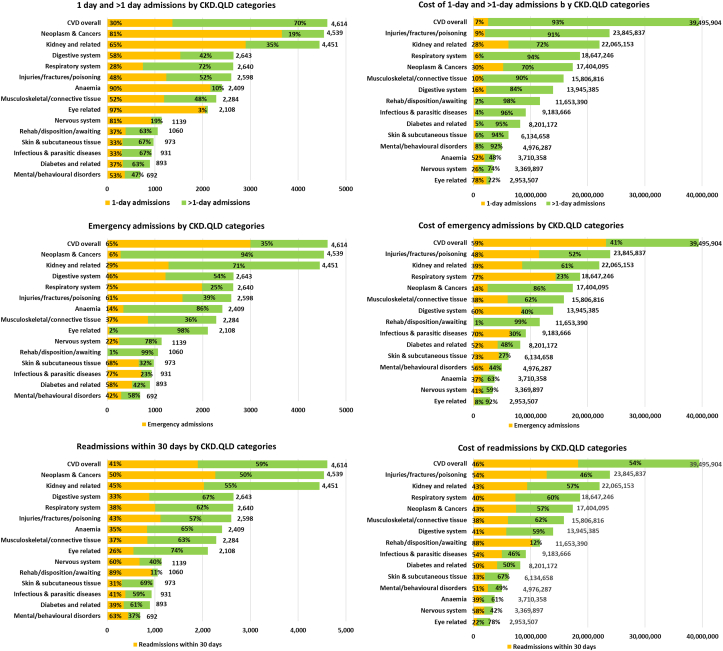
Approximately 81.5% of the patients were admitted at least once, with 42,283 admissions, costing Australian dollars (AUD) 231 million. The average number of admissions per person-year was 1.7, and the cost was AUD 9,060, 10 times and 2 times their Australian averages, respectively. Single (1-day) admissions constituted 59.2% of all the hospital episodes, led by neoplasms (largely chemotherapy), anemia, CKD-related conditions and eye conditions (largely cataract extractions), but only 14.8% of the total costs. Approximately 41% of admissions were >1-day admissions, constituting 85.2% of the total costs, with cardiovascular conditions, respiratory conditions, CKD-related conditions, and injuries, fractures, or poisoning being the dominant causes. Readmission within 30 days of discharge constituted >42% of the admissions and 46.8% costs. Admissions not directly related to CKD constituted 90% of the admissions and costs. More than 40% of the admissions and costs were through the emergency department. Approximately 19% of the hospitalized patients and 27% of the admissions did not have kidney disease mentioned as either principal or associate causes.
Variable follow-up times because of different dates of consent.
The hospital burden of patients with CKD is mainly driven by complex multiday admissions and readmissions involving comorbid conditions, which may not be directly related to their CKD. Strategies to prevent these complex admissions and readmissions should minimize hospital costs and outcomes.
PLAIN-LANGUAGE SUMMARY: We analyzed primary causes, types, and costs of hospitalizations among 7,201 patients with chronic kidney disease (CKD) from renal speciality clinics across Queensland, Australia, over an average follow-up of 3.54 years. The average annual cost per person was $9,060, and was the highest in those with more advanced CKD, higher age, and with diabetes. More than 85% of costs were driven by more complex hospitalizations with longer length of stay. Cardiovascular disease was the single largest contributor for hospitalizations, length of hospital stay, and total costs. Readmission within 30 days of discharge, particularly for the same disorder, and multiday admissions should be the main targets for mitigation of hospital costs in this population.
对于慢性肾脏病(CKD)非透析患者在死亡或开始肾脏替代治疗(KRT)之前的住院情况,人们了解甚少。
回顾性观察队列研究。
对昆士兰州(QLD)10家公立肾脏诊所的7201例CKD患者的住院情况进行研究,这些患者自2011年5月起纳入CKD.QLD登记系统,随访25496.34人年,直至他们开始接受KRT、死亡或至2018年6月30日。
CKD患者的人口统计学和临床特征。
住院情况。
我们评估了人口统计学和临床特征与住院、住院时间和费用之间的关联。
约81.5%的患者至少住院一次,共住院42283次,花费2.31亿澳元。每人每年的平均住院次数为1.7次,费用为9060澳元,分别是澳大利亚平均水平的10倍和2倍。单次(1天)住院占所有住院病例的59.2%,主要由肿瘤(主要是化疗)、贫血、CKD相关疾病和眼部疾病(主要是白内障摘除术)导致,但仅占总费用的14.8%。约41%的住院时间超过1天,占总费用的85.2%,主要病因是心血管疾病、呼吸系统疾病、CKD相关疾病以及损伤、骨折或中毒。出院后30天内再次入院占入院次数的42%以上,费用占46.8%。与CKD无直接关系的住院占住院次数和费用的90%。超过40%的住院次数和费用是通过急诊科产生的。约19%的住院患者和27%的住院病例未将肾脏疾病列为主要或次要病因。
由于同意日期不同,随访时间存在差异。
CKD患者的住院负担主要由涉及合并症的复杂多日住院和再次入院导致,这些合并症可能与他们的CKD无直接关系。预防这些复杂住院和再次入院的策略应能降低医院成本并改善治疗结果。
我们分析了澳大利亚昆士兰州各肾脏专科诊所7201例慢性肾脏病(CKD)患者的住院主要病因、类型和费用,平均随访3.54年。每人每年平均费用为9060美元,在CKD更严重、年龄更大以及患有糖尿病的患者中费用最高。超过85%的费用由住院时间更长的更复杂住院导致。心血管疾病是住院、住院时间和总费用的最大单一贡献因素。出院后30天内再次入院,尤其是因同一疾病再次入院以及多日住院,应成为减轻该人群医院成本的主要目标。