Arnie Charbonneau Cancer Institute, University of Calgary, Calgary, Alberta, Canada.
Sylvester Comprehensive Cancer Center, Miami, FL, USA.
Nat Med. 2023 Sep;29(9):2295-2306. doi: 10.1038/s41591-023-02491-5. Epub 2023 Aug 31.
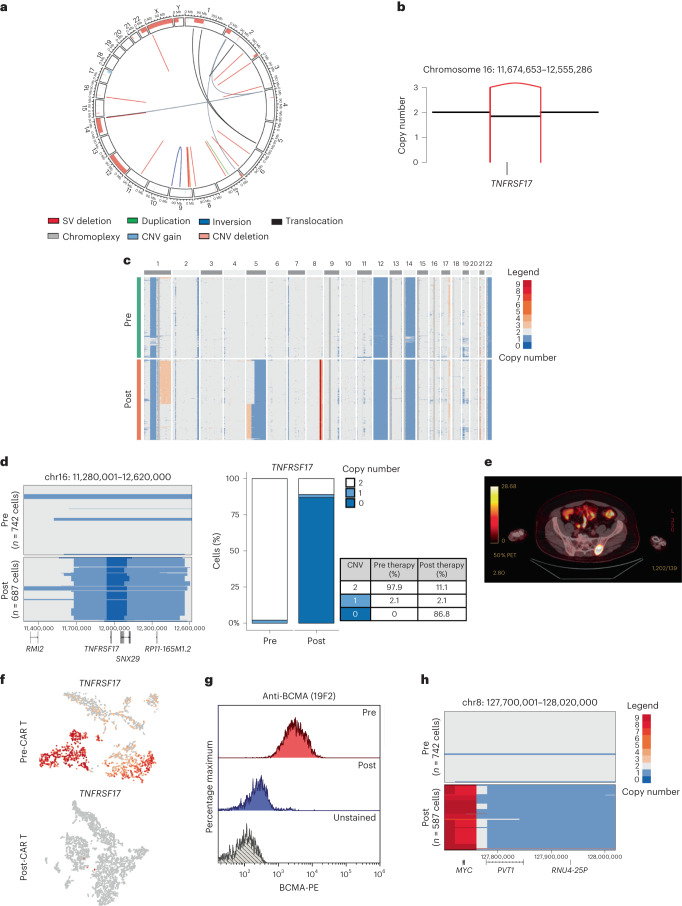
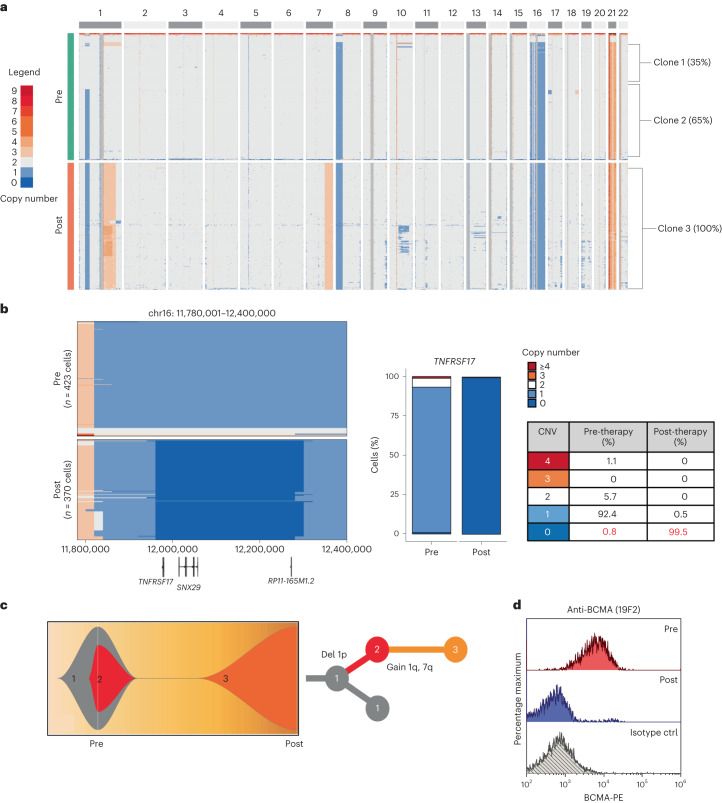
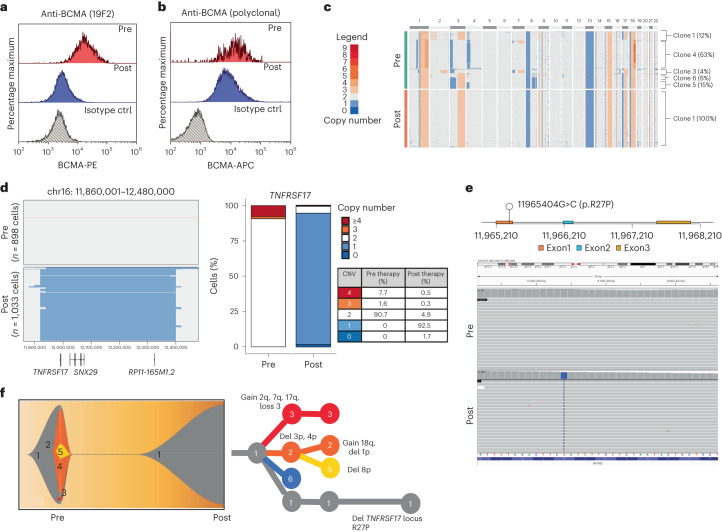
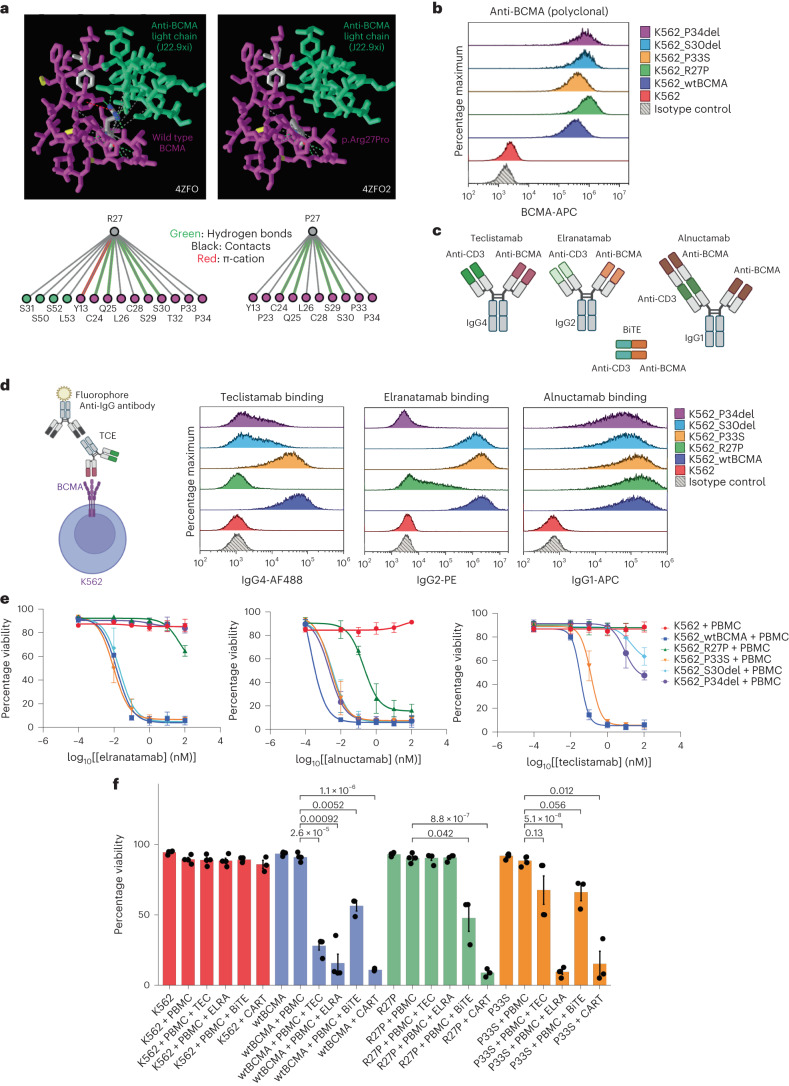
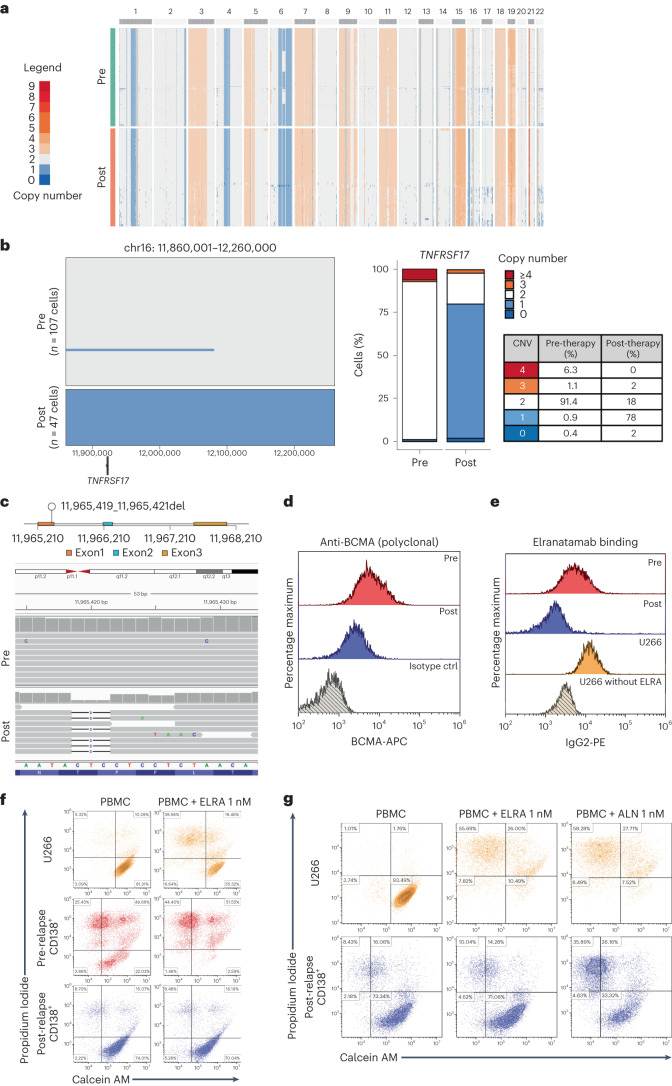
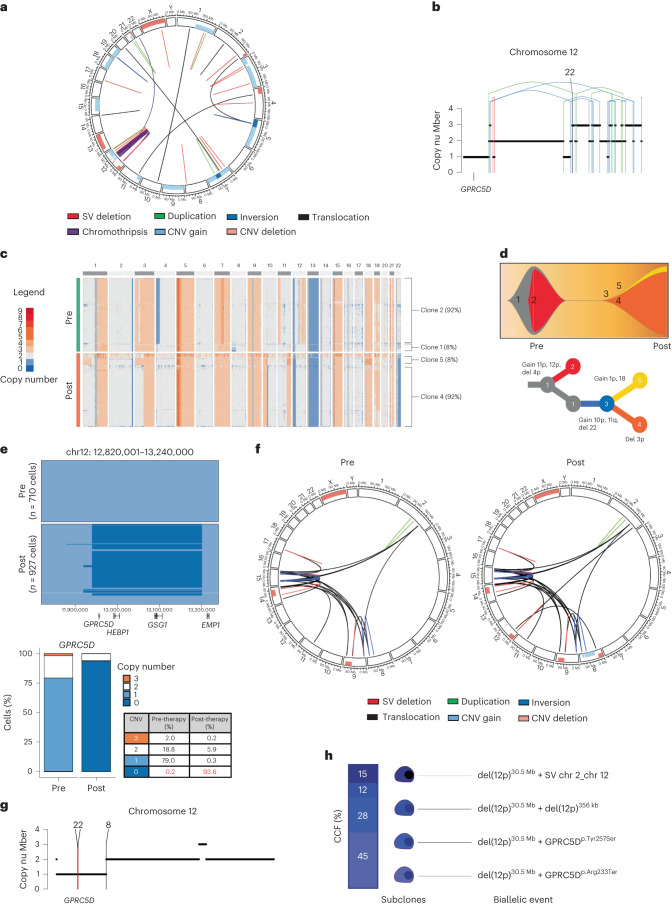
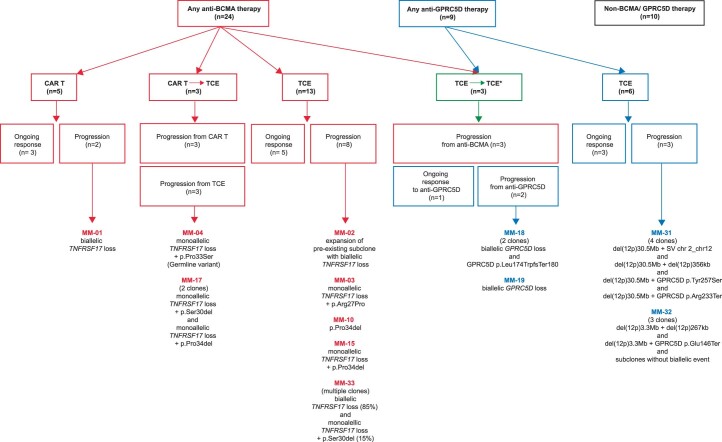
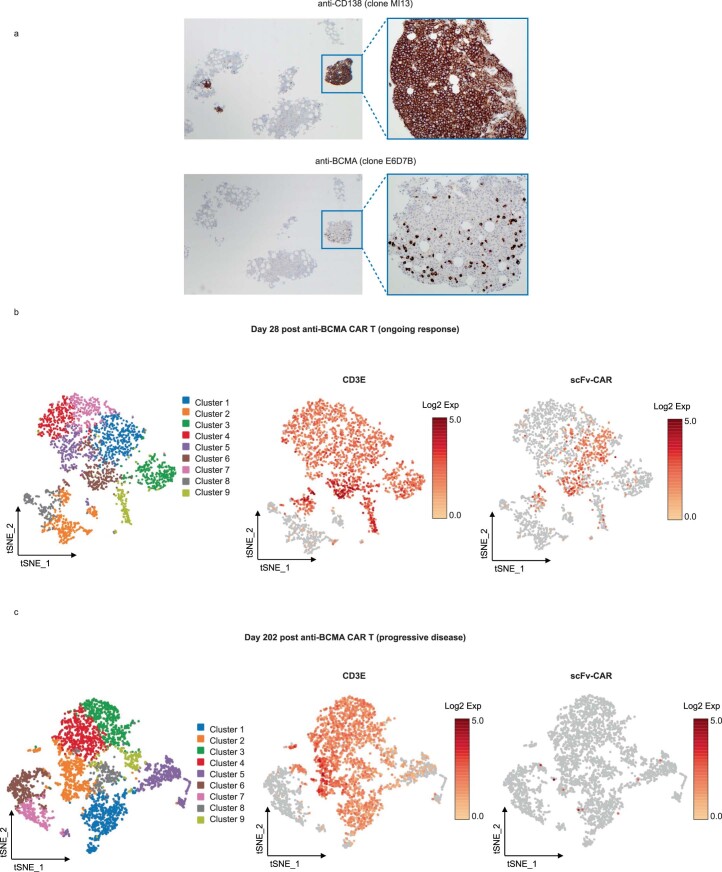
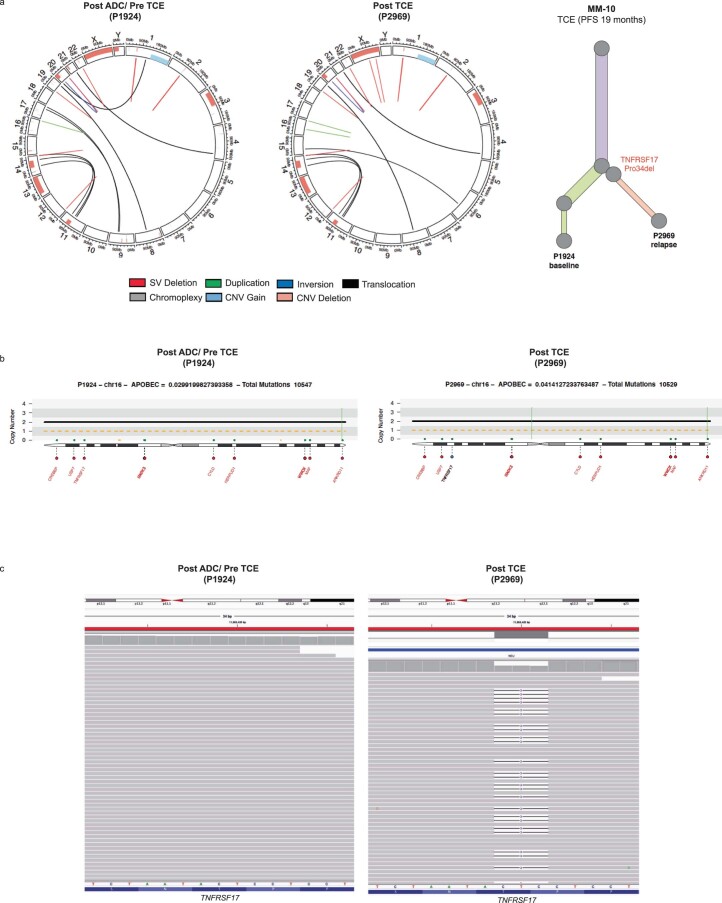
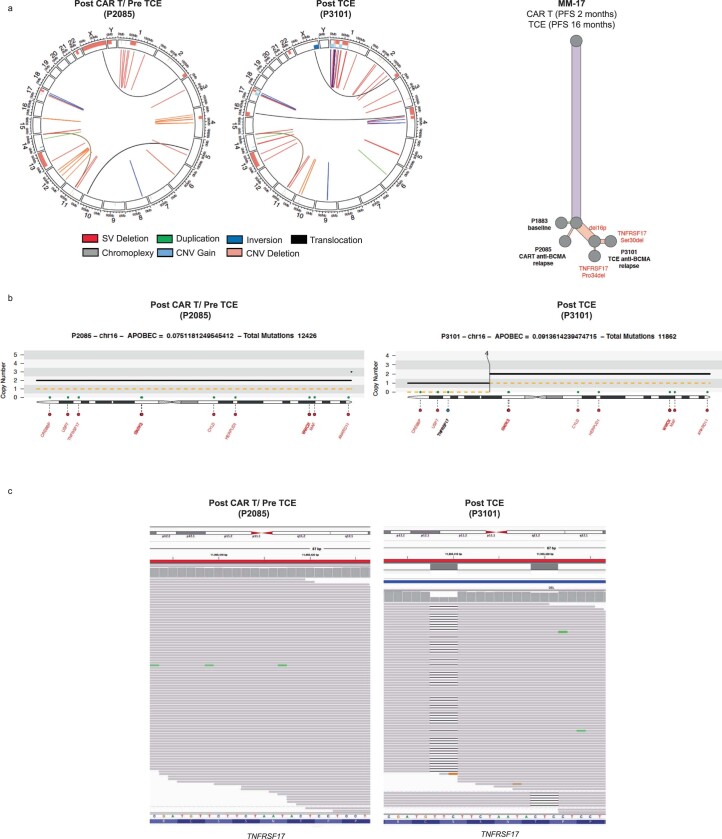
B cell maturation antigen (BCMA) target loss is considered to be a rare event that mediates multiple myeloma (MM) resistance to anti-BCMA chimeric antigen receptor T cell (CAR T) or bispecific T cell engager (TCE) therapies. Emerging data report that downregulation of G-protein-coupled receptor family C group 5 member D (GPRC5D) protein often occurs at relapse after anti-GPRC5D CAR T therapy. To examine the tumor-intrinsic factors that promote MM antigen escape, we performed combined bulk and single-cell whole-genome sequencing and copy number variation analysis of 30 patients treated with anti-BCMA and/or anti-GPRC5D CAR T/TCE therapy. In two cases, MM relapse post-TCE/CAR T therapy was driven by BCMA-negative clones harboring focal biallelic deletions at the TNFRSF17 locus at relapse or by selective expansion of pre-existing subclones with biallelic TNFRSF17 loss. In another five cases of relapse, newly detected, nontruncating, missense mutations or in-frame deletions in the extracellular domain of BCMA negated the efficacies of anti-BCMA TCE therapies, despite detectable surface BCMA protein expression. In the present study, we also report four cases of MM relapse with biallelic mutations of GPRC5D after anti-GPRC5D TCE therapy, including two cases with convergent evolution where multiple subclones lost GPRC5D through somatic events. Immunoselection of BCMA- or GPRC5D-negative or mutant clones is an important tumor-intrinsic driver of relapse post-targeted therapies. Mutational events on BCMA confer distinct sensitivities toward different anti-BCMA therapies, underscoring the importance of considering the tumor antigen landscape for optimal design and selection of targeted immunotherapies in MM.
B 细胞成熟抗原 (BCMA) 靶点丢失被认为是导致多发性骨髓瘤 (MM) 对抗 BCMA 嵌合抗原受体 T 细胞 (CAR T) 或双特异性 T 细胞衔接器 (TCE) 疗法产生耐药的罕见事件。新出现的数据表明,在抗 GPRC5D CAR T 治疗后复发时,G 蛋白偶联受体家族 C 组 5 成员 D (GPRC5D) 蛋白的下调经常发生。为了研究促进 MM 抗原逃逸的肿瘤内在因素,我们对 30 名接受抗 BCMA 和/或抗 GPRC5D CAR T/TCE 治疗的患者进行了合并的 bulk 和单细胞全基因组测序和拷贝数变异分析。在两个病例中,TCE/CAR T 治疗后 MM 复发是由复发时 TNFRSF17 基因座存在焦点双等位基因缺失的 BCMA 阴性克隆或先前存在的具有双等位基因 TNFRSF17 缺失的亚克隆选择性扩增驱动的。在另外五个复发病例中,新检测到的、非截断的、外显子缺失或框内缺失的 BCMA 突变使抗 BCMA TCE 疗法失效,尽管表面仍可检测到 BCMA 蛋白表达。在本研究中,我们还报告了四个在抗 GPRC5D TCE 治疗后发生 GPRC5D 双等位基因突变的 MM 复发病例,包括两个具有多个亚克隆通过体细胞事件丢失 GPRC5D 的趋同进化病例。靶向治疗后 BCMA 或 GPRC5D 阴性或突变克隆的免疫选择是复发的重要肿瘤内在驱动因素。BCMA 上的突变事件赋予其对不同抗 BCMA 疗法的不同敏感性,这凸显了考虑肿瘤抗原图谱对于 MM 中最佳设计和选择靶向免疫疗法的重要性。