Kim Kyu, Cho Iksung, Ko Kyu-Yong, Lee Seung-Hyun, Lee Sak, Hong Geu-Ru, Ha Jong-Won, Shim Chi Young
Division of Cardiology, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea.
Department of Cardiothoracic Surgery, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea.
Korean Circ J. 2023 Nov;53(11):744-755. doi: 10.4070/kcj.2023.0022. Epub 2023 Aug 1.
Aortic valve replacement (AVR) is considered a class I indication for symptomatic severe aortic stenosis (AS). However, there is little evidence regarding the potential benefits of early AVR in symptomatic patients diagnosed with normal-flow, low-gradient (NFLG) severe AS.
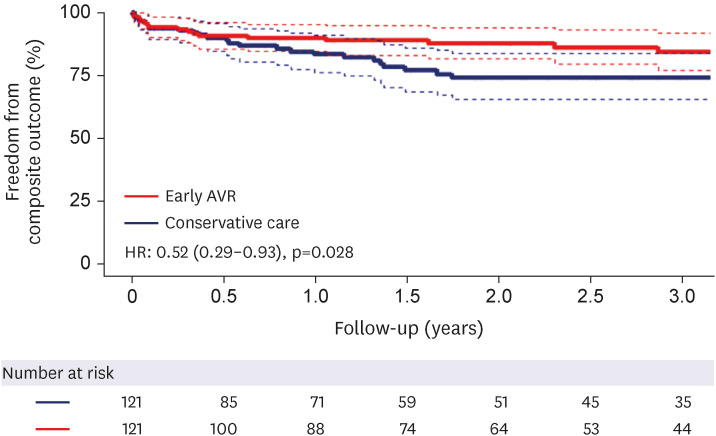
Two-hundred eighty-one patients diagnosed with symptomatic NFLG severe AS (stroke volume index ≥35 mL/m², mean transaortic pressure gradient <40 mmHg, peak transaortic velocity <4 m/s, and aortic valve area <1.0 cm²) between January 2010 and December 2020 were included in this retrospective study. After performing 1:1 propensity score matching, 121 patients aged 75.1±9.8 years (including 63 women) who underwent early AVR within 3 months after index echocardiography, were compared with 121 patients who received conservative care. The primary outcome was a composite of all-cause death and heart failure (HF) hospitalization.
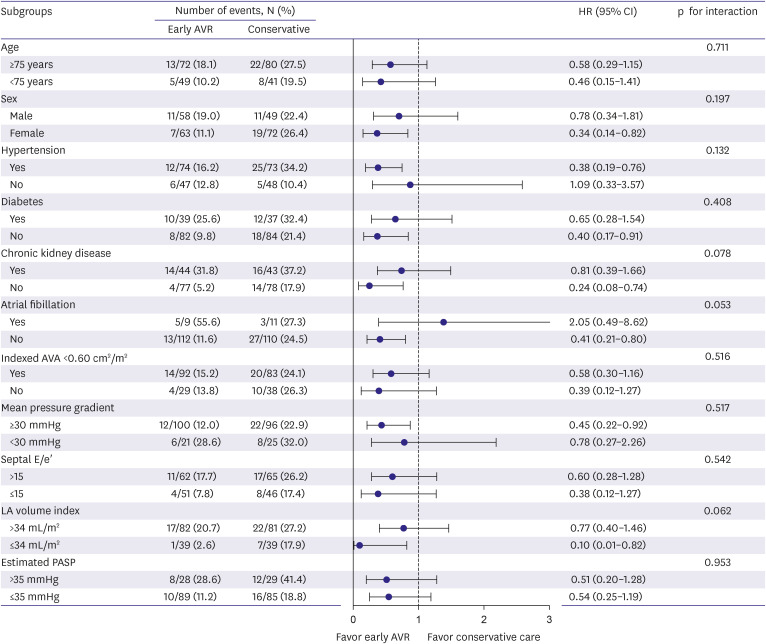
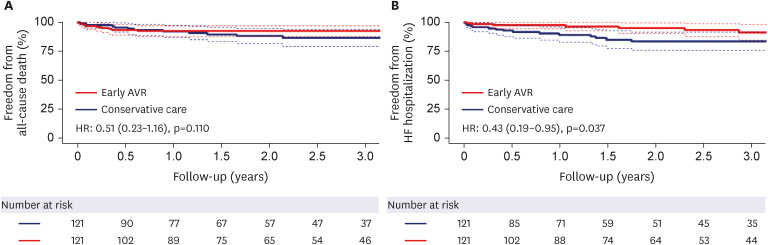
During a median follow-up of 21.9 months, 48 primary outcomes (18 in the early AVR group and 30 in the conservative care group) occurred. The early AVR group demonstrated a significantly lower incidence of primary outcomes (hazard ratio [HR], 0.52; 95% confidence interval [CI], 0.29-0.93; p=0.028); specifically, there was no significant difference in all-cause death (HR, 0.51; 95% CI, 0.23-1.16; p=0.110), although the early AVR group showed a significantly lower incidence of hospitalization for HF (HR, 0.43; 95% CI, 0.19-0.95, p=0.037). Subgroup analyses supported the main findings.
An early AVR strategy may be beneficial in reducing the risk of a composite outcome of death or hospitalization for HF in symptomatic patients with NFLG severe AS. Future randomized studies are required to validate and confirm our findings.
主动脉瓣置换术(AVR)被视为有症状的重度主动脉瓣狭窄(AS)的I类适应症。然而,对于诊断为正常血流、低跨瓣压差(NFLG)的重度AS且有症状的患者,早期AVR潜在益处的证据很少。
本回顾性研究纳入了2010年1月至2020年12月期间诊断为有症状的NFLG重度AS(每搏量指数≥35 mL/m²,平均跨主动脉压力梯度<40 mmHg,峰值跨主动脉速度<4 m/s,主动脉瓣面积<1.0 cm²)的281例患者。在进行1:1倾向评分匹配后,将121例年龄为75.1±9.8岁(包括63名女性)在首次超声心动图检查后3个月内接受早期AVR的患者与121例接受保守治疗的患者进行比较。主要结局是全因死亡和心力衰竭(HF)住院的复合结局。
在中位随访21.9个月期间,发生了48例主要结局(早期AVR组18例,保守治疗组30例)。早期AVR组的主要结局发生率显著较低(风险比[HR],0.52;95%置信区间[CI],0.29 - 0.93;p = 0.028);具体而言,全因死亡无显著差异(HR,0.51;95% CI,0.23 - 1.16;p = 0.110),尽管早期AVR组的HF住院发生率显著较低(HR,0.43;95% CI,0.19 - 0.95,p = 0.037)。亚组分析支持主要研究结果。
早期AVR策略可能有助于降低有症状的NFLG重度AS患者死亡或HF住院复合结局的风险。未来需要进行随机研究来验证和确认我们的研究结果。