Gu Zhangyang, Wu Shengguang, Yang Yu, Ren Tao, Zhang Kai-Wei
Guizhou University of Traditional Chinese Medicine, Guiyang, China.
Department of Orthopaedics, The First Affiliated Hospital of Guizhou University of Traditional Chinese Medicine, Guiyang, China.
Orthop J Sports Med. 2023 Aug 16;11(8):23259671231180854. doi: 10.1177/23259671231180854. eCollection 2023 Aug.
There is no clinical gold standard for the indications for single-row (SR) versus double-row (DR) repair according to small, large, or massive rotator cuff tear size.
To conduct a meta-analysis to compare the clinical outcomes and retear rates after arthroscopic SR and DR repair for rotator cuff injuries with different tear sizes.
Systematic review; Level of evidence, 3.
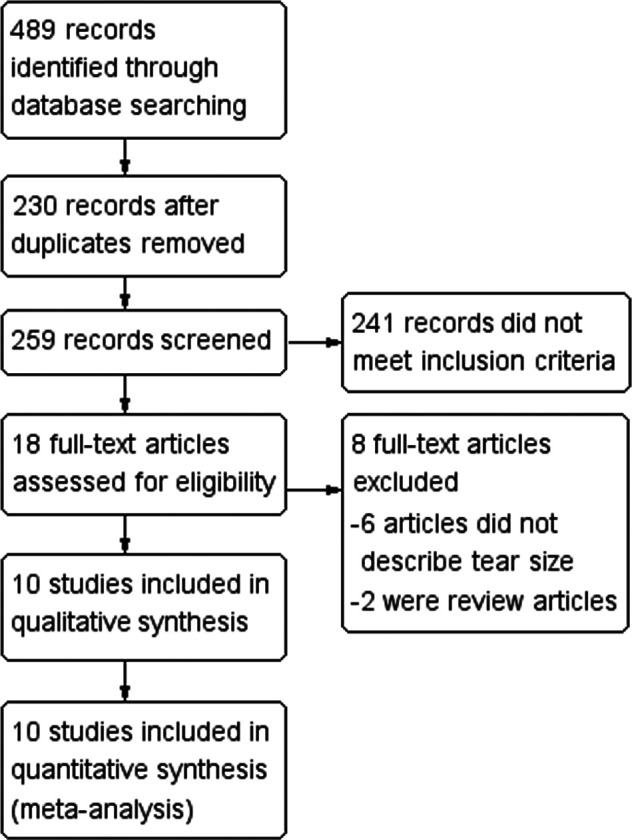
On the basis of PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) criteria, the PubMed, Embase, Cochrane Library databases, Web of Science, China National Knowledge Infrastructure, and China BioMedical Literature database were searched for relevant studies published before November 1, 2021, using the following search terms: "Rotator Cuff Injuries," "Rotator Cuff Tears," "Arthroscopy," "Arthroscopic Surgery," "single-row," and "double-row"; a total of 489 articles were retrieved. Quality evaluation was conducted for all the studies that met the inclusion criteria. This study evaluated the Constant-Murley score, American Shoulder and Elbow Surgeons (ASES) score, University of California, Los Angeles (UCLA) score, and range of motion (ROM) as well as retear rate. A fixed-effects or random-effects model was adopted to calculate the results and assess risk.
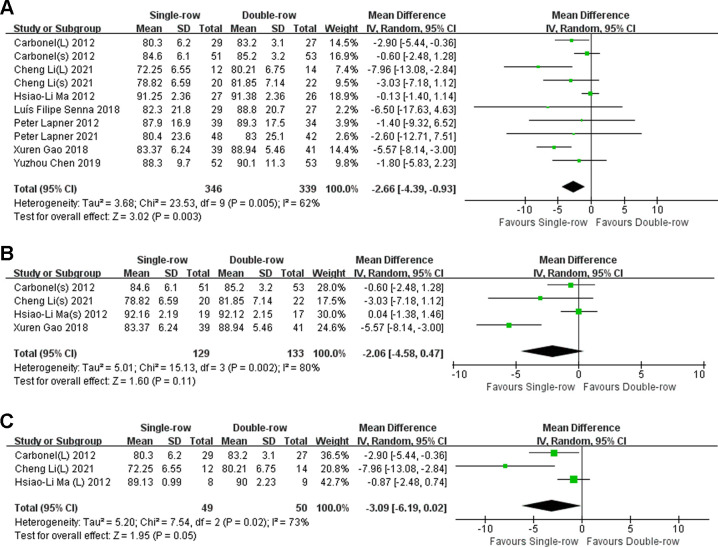
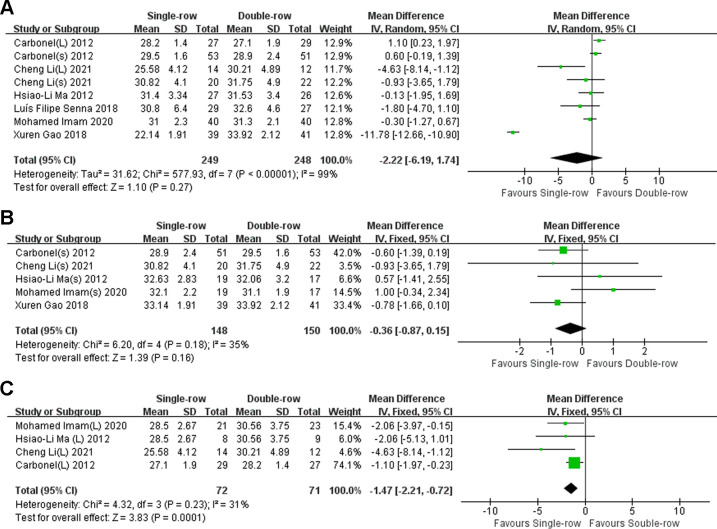
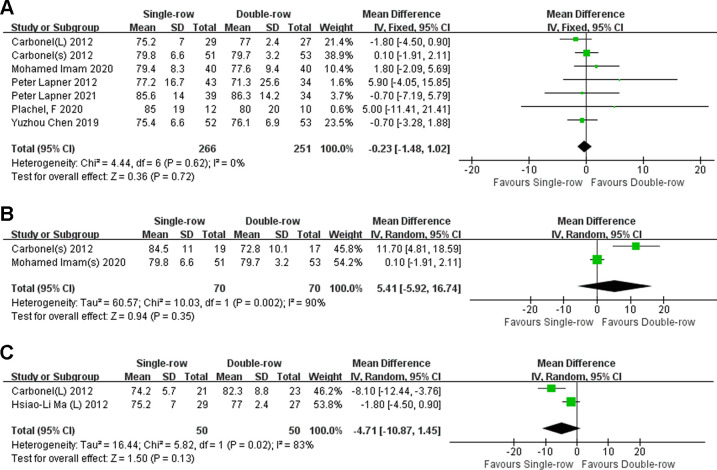
A total of 10 clinical studies were included, with 404 cases of DR and 387 cases of SR. Regarding overall results, DR had better forward elevation ROM (mean difference [MD] = -4.03° [95% CI, -6.00° to -2.06°]; < .0001; = 46%) and a lower retear rate (MD = 2.39 [95% CI, 1.40 to 4.08]; = .001; = 0%) compared with SR repair. With regard to small tears (<3 cm), there was no noticeable difference on any of the 3 outcome scores between SR and DR. For large rotator cuff tears (≥3 cm), DR repair showed significantly better ASES scores (MD = -3.09 [95% CI, -6.19 to 0.02]; = .05; = 73%) and UCLA scores (MD = -1.47 [95% CI, -2.21 to -0.72]; = .0001; = 31%) compared with SR repair.
Our meta-analysis revealed that DR had better UCLA scores, ASES scores, and ROM in forward elevation and lower retear rates. In rotator cuff tears <3 cm, there were no statistical differences in clinical outcome between SR and DR.
对于小、大或巨大肩袖撕裂,单排(SR)修复与双排(DR)修复的适应症尚无临床金标准。
进行一项荟萃分析,比较关节镜下SR和DR修复不同大小肩袖损伤后的临床疗效和再撕裂率。
系统评价;证据等级,3级。
根据PRISMA(系统评价和荟萃分析的首选报告项目)标准,检索PubMed、Embase、Cochrane图书馆数据库、Web of Science、中国知网和中国生物医学文献数据库中2021年11月1日前发表的相关研究,检索词如下:“肩袖损伤”“肩袖撕裂”“关节镜检查”“关节镜手术”“单排”和“双排”;共检索到489篇文章。对所有符合纳入标准的研究进行质量评估。本研究评估了Constant-Murley评分、美国肩肘外科医师(ASES)评分、加利福尼亚大学洛杉矶分校(UCLA)评分、活动范围(ROM)以及再撕裂率。采用固定效应或随机效应模型计算结果并评估风险。
共纳入10项临床研究,其中DR组404例,SR组387例。总体结果显示,与SR修复相比,DR组前屈ROM更好(平均差[MD]=-4.03°[95%CI,-6.00°至-2.06°];P<.0001;I²=46%),再撕裂率更低(MD=2.39[95%CI,1.40至4.08];P=.001;I²=0%)。对于小撕裂(<3 cm),SR和DR在3项结局评分中的任何一项上均无明显差异。对于大肩袖撕裂(≥3 cm),与SR修复相比,DR修复的ASES评分(MD=-3.09[95%CI,-6.19至0.02];P=.05;I²=73%)和UCLA评分(MD=-1.47[95%CI,-2.21至-0.72];P=.0001;I²=31%)显著更好。
我们的荟萃分析显示,DR的UCLA评分、ASES评分、前屈ROM更好,再撕裂率更低。在<3 cm的肩袖撕裂中,SR和DR的临床疗效无统计学差异。