Laboratory of Clinical Investigations, National Institutes of Aging, Baltimore, Md.
Division of Molecular Genetics and Pathology, Center for Devices and Radiological Health, Food and Drug Administration, Silver Spring, Md; Laboratory of Clinical Immunology and Microbiology (LCIM), National Institute of Allergy and Infectious Diseases (NIAID), National Institutes of Health (NIH), Bethesda, Md.
J Allergy Clin Immunol. 2023 Dec;152(6):1619-1633.e11. doi: 10.1016/j.jaci.2023.07.022. Epub 2023 Sep 1.
Chronic granulomatous disease (CGD) is caused by defects in any 1 of the 6 subunits forming the nicotinamide adenine dinucleotide phosphate oxidase complex 2 (NOX2), leading to severely reduced or absent phagocyte-derived reactive oxygen species production. Almost 50% of patients with CGD have inflammatory bowel disease (CGD-IBD). While conventional IBD therapies can treat CGD-IBD, their benefits must be weighed against the risk of infection. Understanding the impact of NOX2 defects on the intestinal microbiota may lead to the identification of novel CGD-IBD treatments.
We sought to identify microbiome and metabolome signatures that can distinguish individuals with CGD and CGD-IBD.
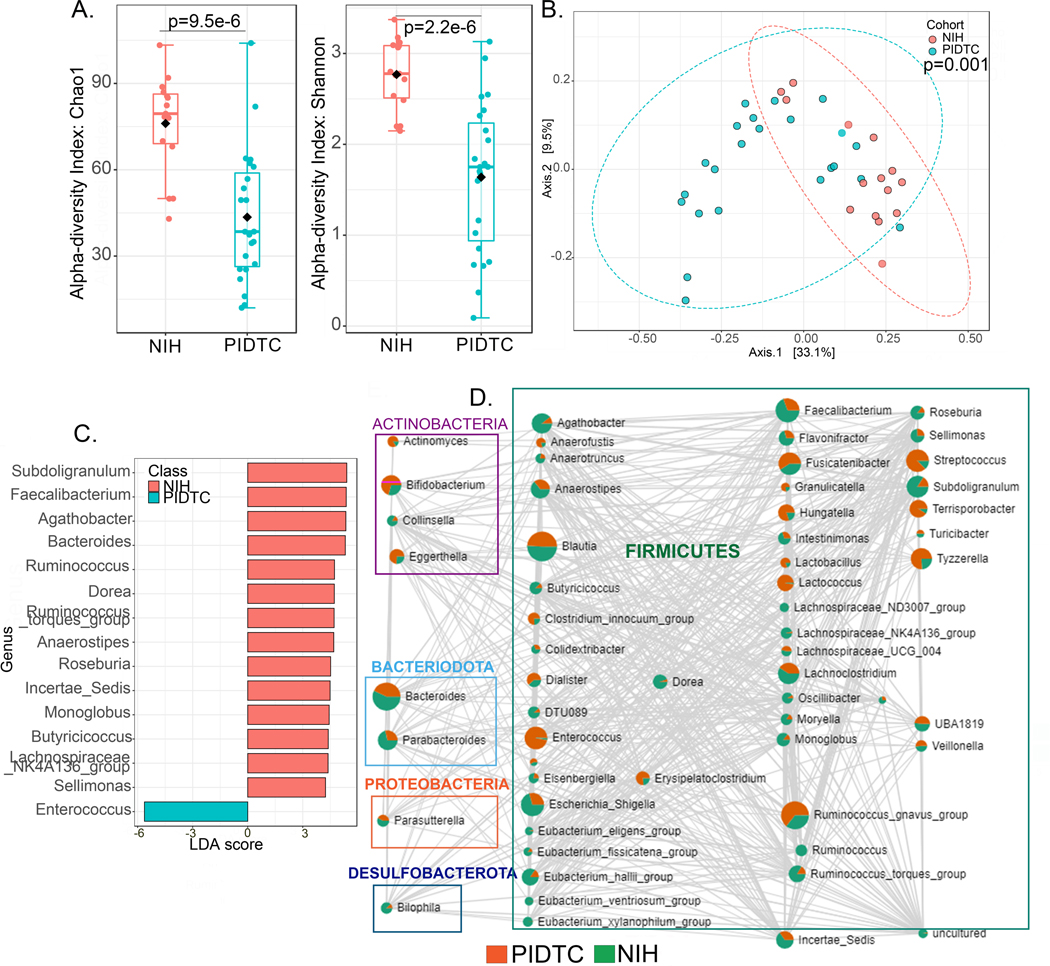
We conducted a cross-sectional observational study of 79 patients with CGD, 8 pathogenic variant carriers, and 19 healthy controls followed at the National Institutes of Health Clinical Center. We profiled the intestinal microbiome (amplicon sequencing) and stool metabolome, and validated our findings in a second cohort of 36 patients with CGD recruited through the Primary Immune Deficiency Treatment Consortium.
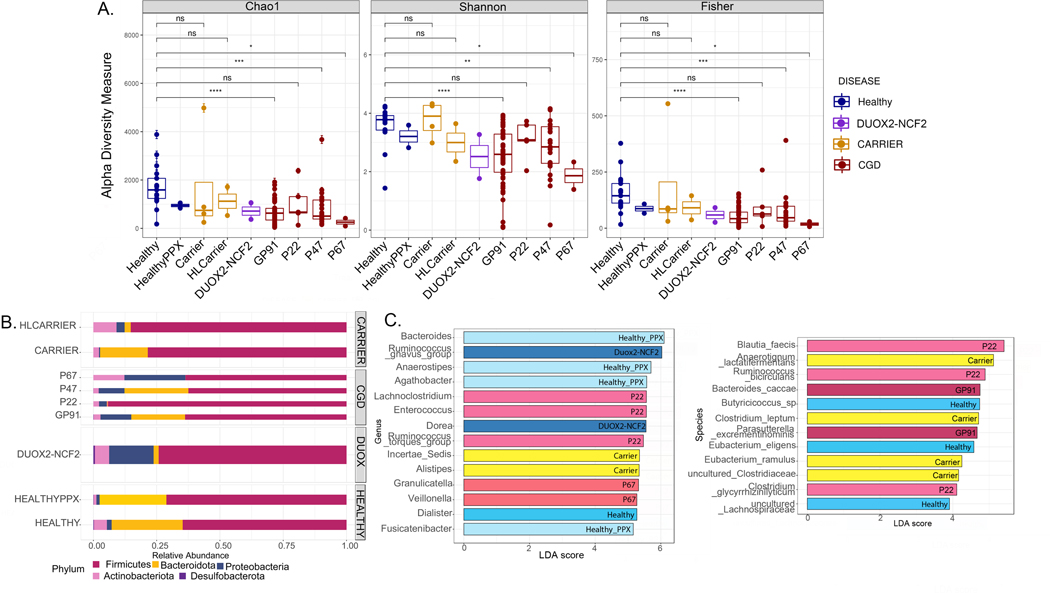
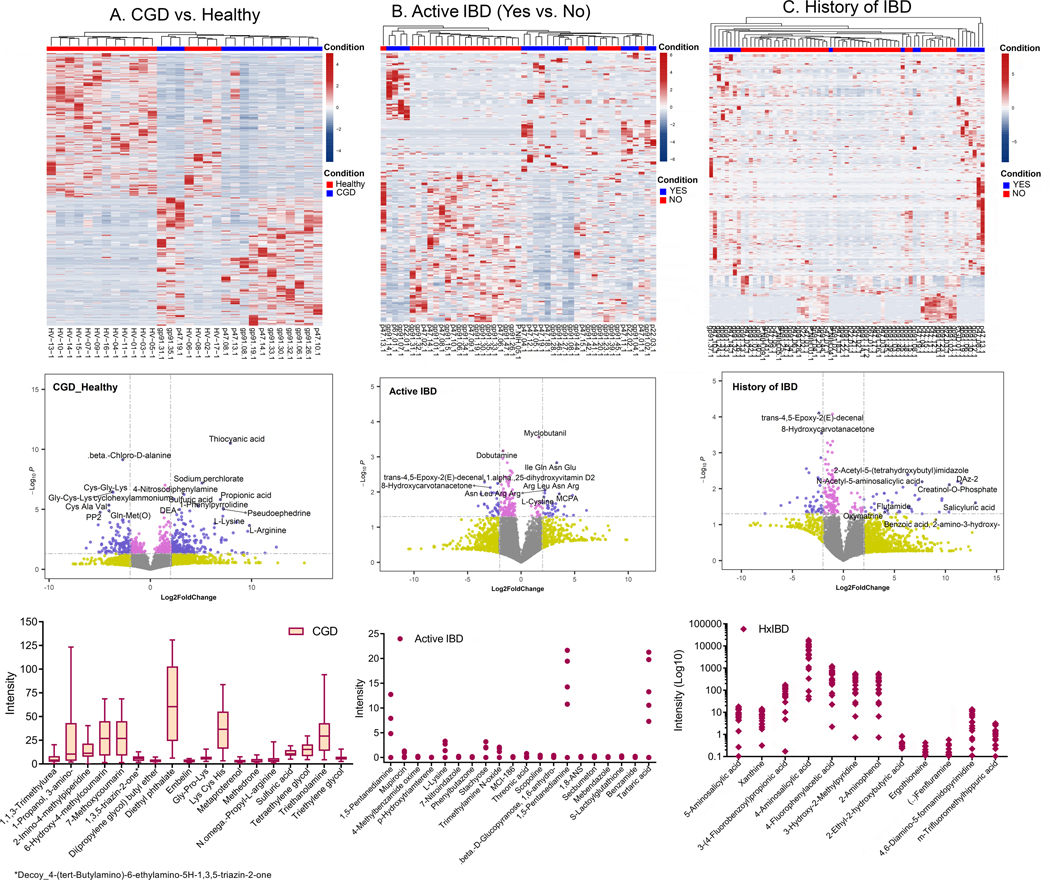
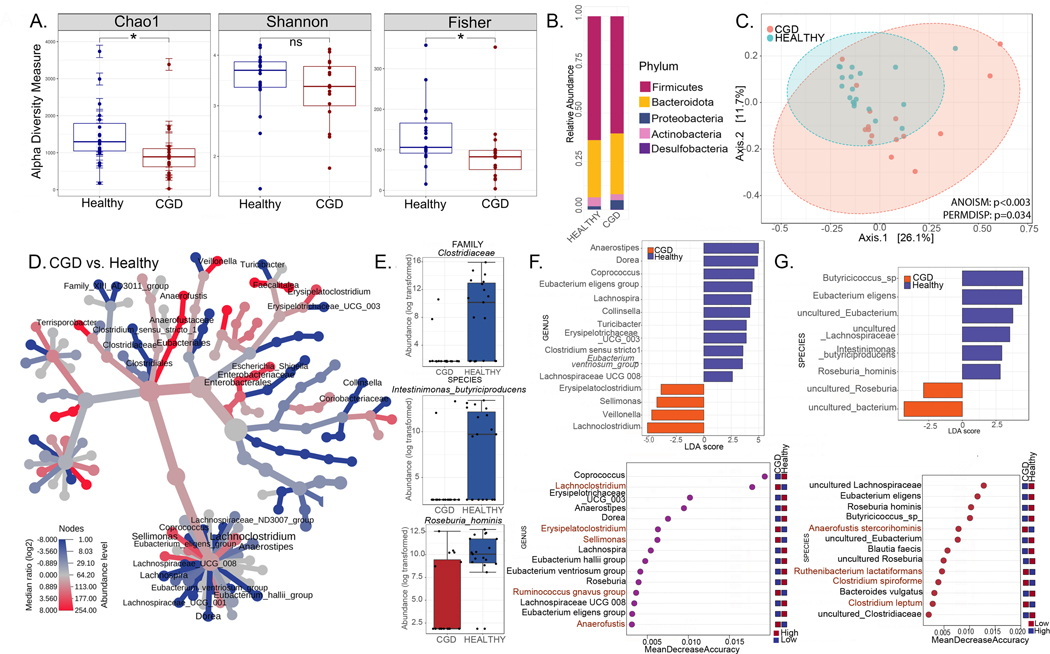
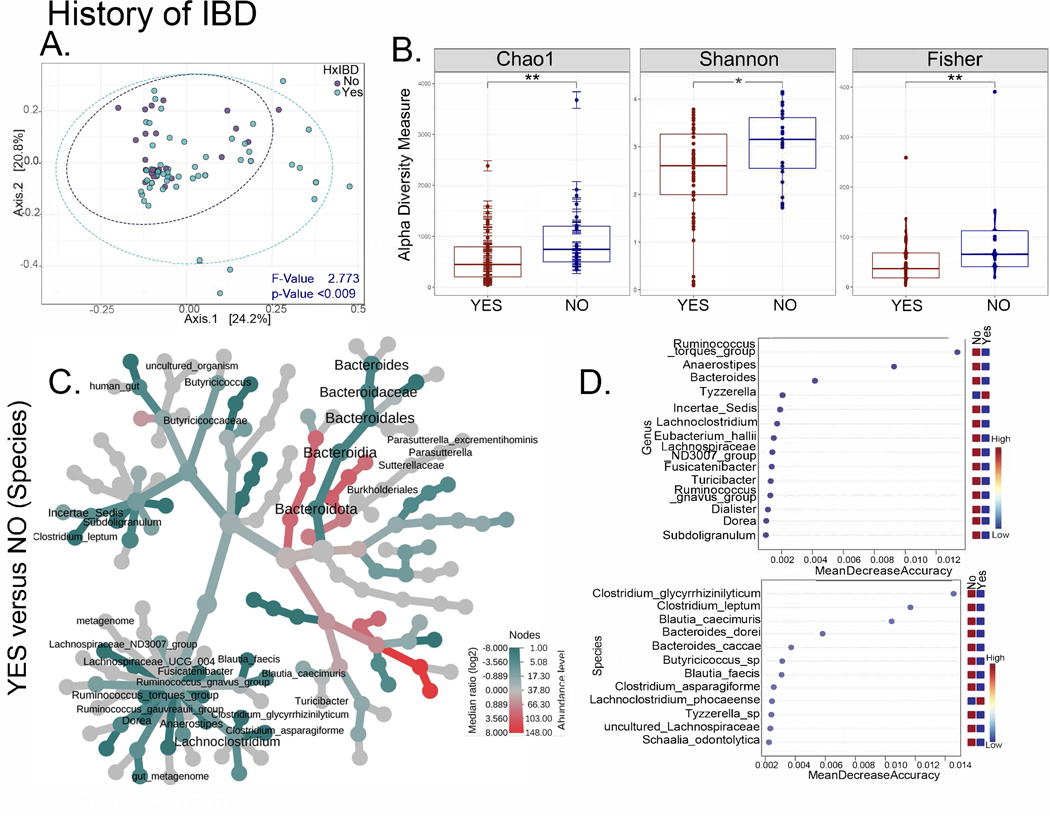
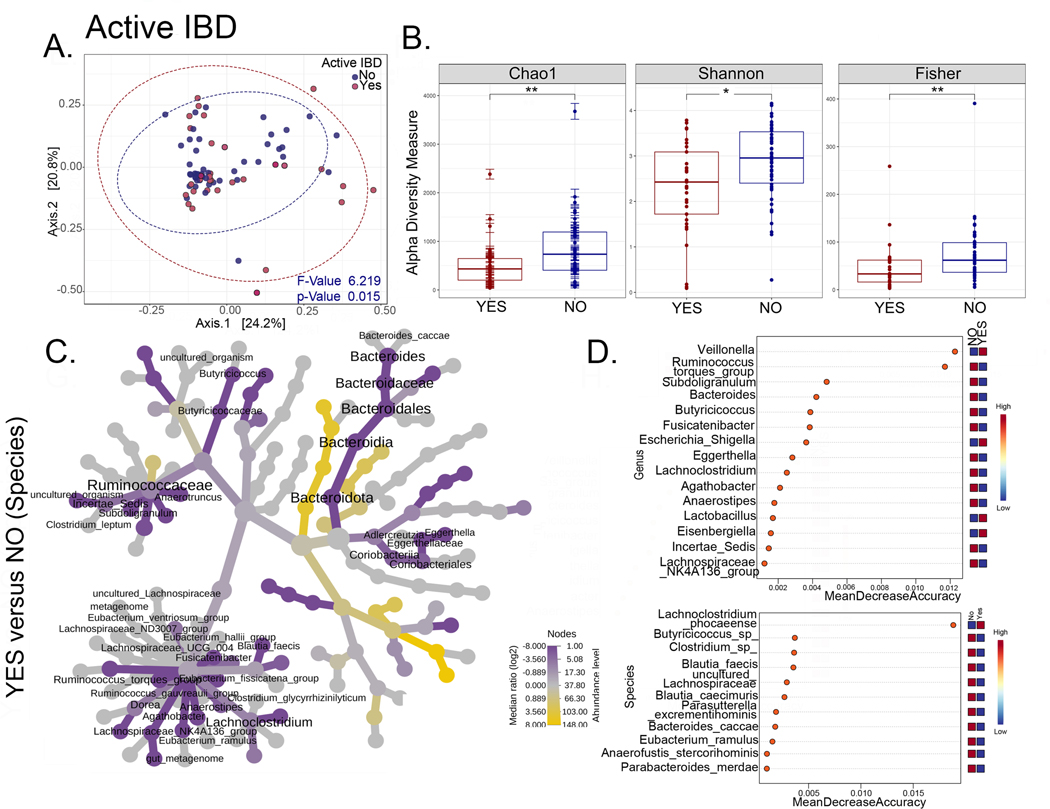
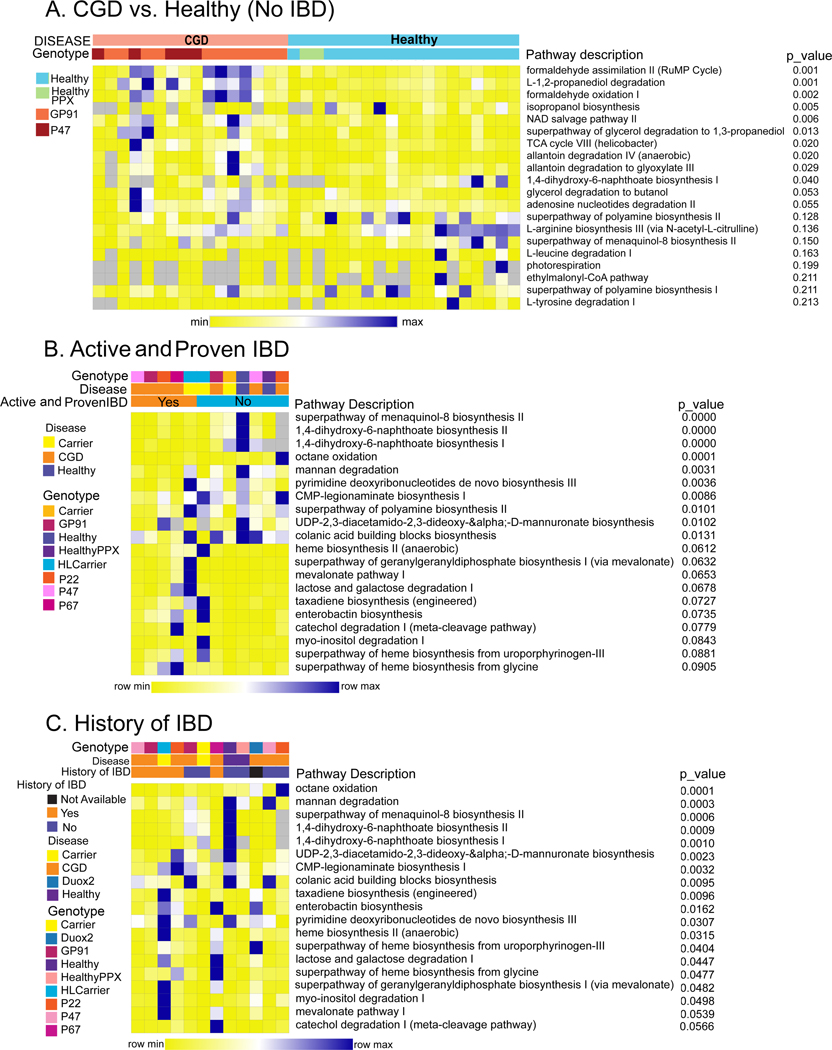
We identified distinct intestinal microbiome and metabolome profiles in patients with CGD compared to healthy individuals. We observed enrichment for Erysipelatoclostridium spp, Sellimonas spp, and Lachnoclostridium spp in CGD stool samples. Despite differences in bacterial alpha and beta diversity between the 2 cohorts, several taxa correlated significantly between both cohorts. We further demonstrated that patients with CGD-IBD have a distinct microbiome and metabolome profile compared to patients without CGD-IBD.
Intestinal microbiome and metabolome signatures distinguished patients with CGD and CGD-IBD, and identified potential biomarkers and therapeutic targets.
慢性肉芽肿病(CGD)是由形成烟酰胺腺嘌呤二核苷酸磷酸氧化酶复合物 2(NOX2)的 6 个亚基中的任何 1 个缺陷引起的,导致吞噬细胞衍生的活性氧产生严重减少或缺失。近 50%的 CGD 患者患有炎症性肠病(CGD-IBD)。虽然常规 IBD 疗法可以治疗 CGD-IBD,但必须权衡其益处与感染风险。了解 NOX2 缺陷对肠道微生物组的影响可能会导致发现新的 CGD-IBD 治疗方法。
我们旨在确定可以区分 CGD 患者和 CGD-IBD 患者的微生物组和代谢组特征。
我们对在国立卫生研究院临床中心接受治疗的 79 名 CGD 患者、8 名致病性变异携带者和 19 名健康对照进行了横断面观察性研究。我们对肠道微生物组(扩增子测序)和粪便代谢组进行了分析,并在通过原发性免疫缺陷治疗联盟招募的 36 名 CGD 患者的第二队列中验证了我们的发现。
与健康个体相比,我们在 CGD 患者中发现了独特的肠道微生物组和代谢组特征。我们观察到 CGD 粪便样本中 Erysipelatoclostridium spp、Sellimonas spp 和 Lachnoclostridium spp 的富集。尽管两个队列的细菌 alpha 和 beta 多样性存在差异,但几个分类群在两个队列之间存在显著相关性。我们进一步证明,CGD-IBD 患者的微生物组和代谢组特征与无 CGD-IBD 的患者不同。
肠道微生物组和代谢组特征可区分 CGD 患者和 CGD-IBD 患者,并确定了潜在的生物标志物和治疗靶点。