Bennett Paige, Tomas Maria Bernadette, Koch Christopher F, Nichols Kenneth J, Palestro Christopher J
Department of Radiology, LIJMC Northwell Health, New Hyde Park, NY 11040, United States.
Department of Radiology, Zucker School of Medicine at Hofstra/Northwell, Hempstead, NY 11549, United States.
World J Radiol. 2023 Aug 28;15(8):241-249. doi: 10.4329/wjr.v15.i8.241.
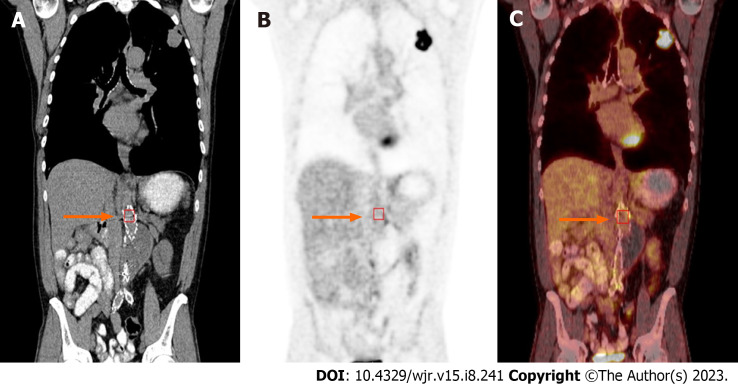
Diagnosis of prosthetic vascular graft infection with [(18)F]fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) allows for early detection of functional changes associated with infection, based on increased glucose utilization by activated macrophages and granulocytes. Aseptic vascular grafts, like all foreign bodies, can stimulate an inflammatory response, which can present as increased activity on 18F-FDG PET/CT. Consequently, distinguishing aseptic inflammation from graft infection, though important, can be difficult. In the case of endovascular aneurysm repair (EVAR), a minimally invasive procedure involving the transfemoral insertion of an endoprosthetic stent graft, the normal postoperative appearance of these grafts on 18F-FDG PET/CT can vary over time, potentially confounding study interpretation.
To investigate the visual, semiquantitative, and temporal characteristics of aseptic vascular grafts in patients status post EVAR.
In this observational retrospective cohort study, patients with history of EVAR who underwent 18F-FDG PET/CT for indications other than infection were identified retrospectively. All patients were asymptomatic for graft infection - no abdominal pain, fever of unknown origin, sepsis, or leukocytosis - at the time of imaging and for ≥ 2 mo after each PET/CT. Imaging studies such as CT for each patient were also reviewed, and any patients with suspected or confirmed vascular graft infection were excluded. One hundred two scans performed on 43 patients (34 males; 9 females; age = 77 ± 8 years at the time of the final PET/CT) were retrospectively reviewed. All 43 patients had an abdominal aortic (AA) vascular graft, 40 patients had a right iliac (RI) limb graft, and 41 patients had a left iliac (LI) limb graft. Twenty-two patients had 1 PET/CT and 21 patients had from 2 to 9 PET/CTs. Grafts were imaged between 2 mo to 168 mo (about 14 years) post placement. Eight grafts were imaged within 6 mo of placement, including three that were imaged within three months of placement. The mean interval between graft placement and PET/CT for all 102 scans was 51 ± 39 mo. PET/CT data was reconstructed with region-of-interest analysis of proximal, mid and distal portions of the grafts and background ascending aorta. Maximum standardized uptake value (SUV) was recorded for each region. SUV-to-background uptake ratios (URs) were calculated. Visual assessment was performed using a 2-pattern grading scale: Diffuse (homogeneous uptake less than liver uptake) and focal (one or more areas of focal uptake in any part of the graft). Statistical analysis was performed.
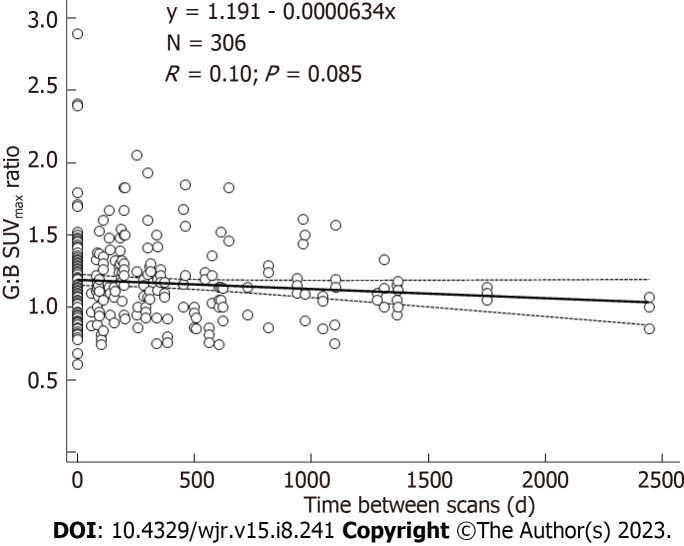
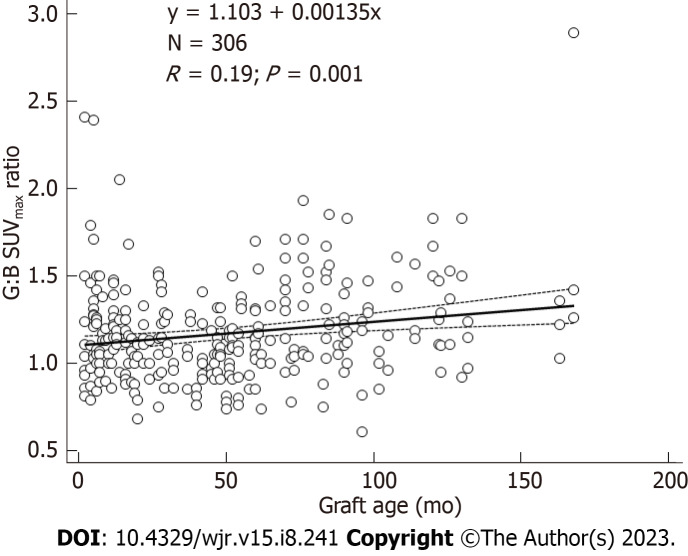
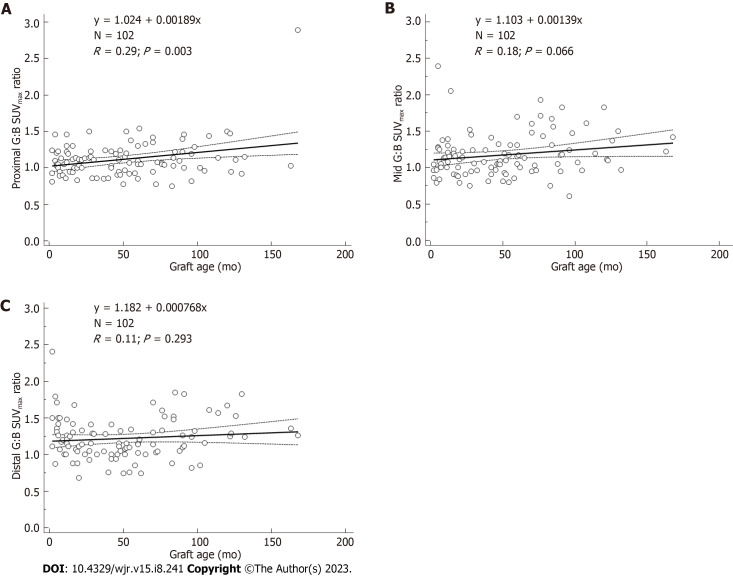
In total, there were 306 AA grafts, 285 LI grafts, 282 RI grafts, and 306 ascending aorta background SUV measurements. For all 102 scans, mean SUV values for AA grafts were 2.8-3.0 along proximal, mid, and distal segments. Mean SUV values for LI grafts and RI grafts were 2.7-2.8. Mean SUV values for background were 2.5 ± 0.5. Mean URs were 1.1-1.2. Visual analysis of the scans reflected results of quantitative analysis. On visual inspection, 98% revealed diffuse, homogeneous 18F-FDG uptake less than liver. Graft URs and visual pattern categories were significantly associated for AA graft URs (F-ratio = 21.5, 0.001), LI graft URs (F-ratio = 20.4, 0.001), and RI graft URs (F-ratio = 30.4, 0.001). Thus, visual patterns of 18F-FDG uptake corresponded statistically significantly to semiquantitative URs. The age of grafts showing focal patterns was greater than grafts showing diffuse patterns, 87 ± 89 50 ± 37 mo, respectively ( = 0.02). URs were significantly associated with graft age for AA grafts ( = 0.19, = 0.001). URs were also significantly associated with graft age for LI grafts ( = 0.25, < 0.0001), and RI grafts ( = 0.31, < 0.001). Quartiles of similar numbers of graft ( = 25-27) grouped by graft age indicated that URs were significantly higher for 4 quartile 2 quartile URs (F-ratio = 19.5, 0.001). When evaluating URs, graft SUVmax values within 10%-20% of the ascending aorta SUV is evident in aseptic grafts, except for grafts in the oldest quartiles. In this study, grafts in the oldest quartiles (> 7 years post EVAR) showed SUV up to 30% higher than the ascending aorta SUV.
Characteristics of an aseptic vascular stent graft in the aorta and iliac vessels on 18F-FDG PET/CT include graft SUV values within 10%-20% of the ascending aorta background SUV. The SUV of older aseptic grafts can be as much as 30% above background. The visual uptake pattern of diffuse, homogeneous uptake less than liver was seen in 98% of aseptic vascular grafts, making this pattern particularly reassuring for clinicians.
使用[¹⁸F]氟脱氧葡萄糖正电子发射断层扫描/计算机断层扫描(¹⁸F-FDG PET/CT)诊断人工血管移植物感染,基于活化巨噬细胞和粒细胞对葡萄糖利用增加,能够早期检测与感染相关的功能变化。无菌血管移植物与所有异物一样,可刺激炎症反应,在¹⁸F-FDG PET/CT上可表现为活性增加。因此,区分无菌性炎症与移植物感染虽然很重要,但可能具有挑战性。在血管内动脉瘤修复术(EVAR)中,这是一种涉及经股动脉插入腔内人工血管支架的微创手术,这些移植物在¹⁸F-FDG PET/CT上的正常术后表现会随时间变化,这可能会混淆研究结果的解读。
研究接受EVAR术后患者的无菌性血管移植物的视觉、半定量和时间特征。
在这项观察性回顾性队列研究中,对有EVAR病史且因非感染指征接受¹⁸F-FDG PET/CT检查的患者进行回顾性识别。所有患者在成像时以及每次PET/CT检查后≥2个月均无移植物感染症状——无腹痛、不明原因发热、败血症或白细胞增多。还对每位患者的CT等影像学检查进行了回顾,并排除了任何疑似或确诊血管移植物感染的患者。对43例患者(34例男性;9例女性;最后一次PET/CT检查时年龄为77±8岁)进行的102次扫描进行了回顾性分析。所有43例患者均有腹主动脉(AA)血管移植物,40例患者有右髂(RI)肢体移植物,41例患者有左髂(LI)肢体移植物。22例患者进行了1次PET/CT检查,21例患者进行了2至9次PET/CT检查。移植物在植入后2个月至168个月(约14年)进行成像。8例移植物在植入后6个月内成像,其中3例在植入后3个月内成像。所有102次扫描中移植物植入与PET/CT检查的平均间隔时间为51±39个月。PET/CT数据通过对移植物近端、中段和远端以及背景升主动脉进行感兴趣区分析进行重建。记录每个区域的最大标准化摄取值(SUV)。计算SUV与背景摄取比值(UR)。使用2种模式分级量表进行视觉评估:弥漫性(均匀摄取低于肝脏摄取)和局灶性(移植物任何部位有一个或多个局灶性摄取区域)。进行了统计分析。
总共对306个AA移植物、285个LI移植物、282个RI移植物以及306个升主动脉背景SUV测量值进行了分析。在所有102次扫描中,AA移植物近端、中段和远端节段的平均SUV值为2.8 - 3.0。LI移植物和RI移植物的平均SUV值为2.7 - 2.8。背景的平均SUV值为2.5±0.5。平均UR为1.1 - 1.2。扫描的视觉分析反映了定量分析结果。在视觉检查中,98%显示弥漫性、均匀的¹⁸F-FDG摄取低于肝脏。AA移植物UR(F值 = 21.5,P = 0.001)、LI移植物UR(F值 = 20.4,P = 0.001)和RI移植物UR(F值 = 30.4,P = 0.001)的移植物UR与视觉模式类别显著相关。因此,¹⁸F-FDG摄取的视觉模式在统计学上与半定量UR显著对应。显示局灶性模式的移植物年龄大于显示弥漫性模式的移植物,分别为87±89个月和50±37个月(P = 0.02)。AA移植物的UR与移植物年龄显著相关(r = 0.19,P = 0.001)。LI移植物的UR也与移植物年龄显著相关(r = 0.25,P < 0.0001),RI移植物的UR与移植物年龄显著相关(r = 0.31,P < 0.001)。按移植物年龄分组的相似数量移植物(n = 25 - 27)四分位数表明,第4四分位数的UR显著高于第2四分位数的UR(F值 = 19.5,P = 0.001)。在评估UR时,除了最老四分位数的移植物外,无菌移植物中移植物SUVmax值在升主动脉SUV的10% - 20%范围内是明显的。在本研究中,最老四分位数(EVAR术后>7年)的移植物显示SUV比升主动脉SUV高30%。
¹⁸F-FDG PET/CT上主动脉和髂血管中无菌性血管支架移植物的特征包括移植物SUV值在升主动脉背景SUV的10% - 20%范围内。较老无菌移植物的SUV可比背景高30%。98%的无菌血管移植物可见弥漫性、均匀摄取低于肝脏的视觉摄取模式,这一模式对临床医生特别有参考价值。