Department of Medicine, Division of Palliative Care, University of Ottawa, Ottawa, Ontario, Canada
Ottawa Hospital Research Institute, Ottawa, Ontario, Canada.
BMJ Open. 2023 Sep 5;13(9):e075518. doi: 10.1136/bmjopen-2023-075518.
To compare comorbidities, symptoms and end-of-life (EoL) palliative medication (antisecretories, opioids, antipsychotics and sedatives) use among decedents before and during the COVID-19 pandemic.
In a retrospective cohort study, decedent records in three acute care hospitals were abstracted, generating a prepandemic (November 2019-February 2020) group (pre-COVID) and two intrapandemic (March-August 2020, wave 1) groups, one without (COVID-ve) and one with COVID-19 infection (COVID+ve). Control group decedents were matched 2:1 on age, sex and care service (medicine/intensive care unit (ICU)) with COVID+ve decedents.
Three regional acute care teaching hospitals in Ottawa, Canada PARTICIPANTS: Decedents (N=425): COVID+ve (n=85), COVID-ve (n=170) and pre-COVID (n=170).
Data were abstracted regarding demographics, admission comorbidities and symptoms, and EoL medication use; opioid doses were standardised to parenteral morphine equivalent daily dose (MEDD), and the predictors of upper quartile MEDD in the last 24 hours of life were examined in multivariable logistic regression with adjusted ORs (aORs) and 95% CIs.
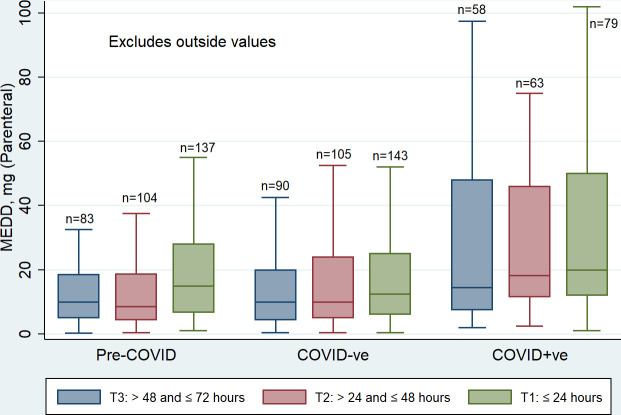
The prevalence of dementia (41% vs 28% and 26%, p=0.03), breathlessness (63.5% vs 42% and 47%, p<0.01), cough (40% vs 27% and 19%, p<0.01) and fever (54% vs 9% and 13.5%) was higher in COVID+ve versus pre-COVID and COVID-ve groups, respectively. The median (IQR) of MEDD over the last 72 hours of life was 16.7 (9-36.5) vs 13.5 (5.7-21.8) and 10.5 (5.3-23.8) for COVID+ve versus pre-COVID and COVID-ve groups, respectively, (p=0.007). Male sex, COVID+ve grouping, ICU death and high-flow nasal cannula use predicted upper quartile MEDD dose, aORs (95% CIs): 1.84 (1.05 to 3.22), 2.62 (1.29 to 5.3), 5.14 (2.47 to 10.7) and 1.93 (1.05 to 3.52), respectively. COVID+ve group decedents used highest lorazepam and propofol doses.
COVID-19 decedents, particularly those in ICU, required higher EoL opioid and sedating medication doses than matched prepandemic or intrapandemic controls. These findings should inform and guide clinical practice.
比较 COVID-19 大流行前后死亡患者的合并症、症状和临终(EoL)姑息治疗药物(止吐药、阿片类药物、抗精神病药和镇静剂)的使用情况。
在一项回顾性队列研究中,从三家急性护理医院的死亡记录中提取数据,生成一个大流行前(2019 年 11 月至 2020 年 2 月)组(前 COVID 组)和两个大流行内(2020 年 3 月至 8 月,第 1 波)组,一组无 COVID-19 感染(COVID-ve),一组有 COVID-19 感染(COVID+ve)。COVID+ve 死亡患者与 COVID+ve 死亡患者按年龄、性别和护理服务(内科/重症监护病房(ICU))进行 2:1 匹配。
加拿大渥太华的三个区域性急性护理教学医院
死亡患者(N=425):COVID+ve(n=85)、COVID-ve(n=170)和前 COVID 组(n=170)。
数据摘要包括人口统计学、入院合并症和症状以及 EoL 药物使用情况;阿片类药物剂量标准化为肠胃外吗啡等效日剂量(MEDD),并在多变量逻辑回归中检查最后 24 小时生命 MEDD 上四分位数的预测因素,使用调整后的比值比(aOR)和 95%置信区间(CI)。
与前 COVID 组和 COVID-ve 组相比,COVID+ve 组痴呆(41% vs 28% 和 26%,p=0.03)、呼吸困难(63.5% vs 42% 和 47%,p<0.01)、咳嗽(40% vs 27% 和 19%,p<0.01)和发热(54% vs 9%和 13.5%,p<0.01)的发生率更高。COVID+ve 组与前 COVID 组和 COVID-ve 组相比,最后 72 小时 MEDD 的中位数(IQR)分别为 16.7(9-36.5)、13.5(5.7-21.8)和 10.5(5.3-23.8)(p=0.007)。男性、COVID+ve 分组、ICU 死亡和高流量鼻导管使用预测 MEDD 剂量的上四分位数,aOR(95%CI):1.84(1.05 至 3.22)、2.62(1.29 至 5.3)、5.14(2.47 至 10.7)和 1.93(1.05 至 3.52),分别。COVID+ve 组死亡患者使用了最高剂量的劳拉西泮和丙泊酚。
COVID-19 死亡患者,特别是 ICU 死亡患者,临终前需要更高剂量的阿片类药物和镇静药物,与匹配的大流行前或大流行内对照组相比。这些发现应告知并指导临床实践。