Division of Infectious Diseases, School of Medicine, Washington University in St. Louis, St. Louis, USA.
Department of Epidemiology, Gillings School of Global Public Health, University of North Carolina at Chapel Hill, Chapel Hill, NC, USA.
BMC Public Health. 2023 Sep 5;23(1):1724. doi: 10.1186/s12889-023-16353-9.
Little is known about the effects of universal test and treat (UTT) policies on HIV care outcomes among youth living with HIV (YLHIV). Moreover, there is a paucity of information regarding when YLHIV are most susceptible to disengagement from care under the newest treatment guidelines. The longitudinal HIV care continuum is an underutilized tool that can provide a holistic understanding of population-level HIV care trajectories and be used to compare treatment outcomes across groups. We aimed to explore effects of the UTT policy on longitudinal outcomes among South African YLHIV and identify temporally precise opportunities for re-engaging this priority population in the UTT era.
Using medical record data, we conducted a retrospective cohort study among youth aged 18-24 diagnosed with HIV from August 2015-December 2018 in nine health care facilities in South Africa. We used Fine and Gray sub-distribution proportional hazards models to characterize longitudinal care continuum outcomes in the population overall and stratified by treatment era of diagnosis. We estimated the proportion of individuals in each stage of the continuum over time and the restricted mean time spent in each stage in the first year following diagnosis. Sub-group estimates were compared using differences.
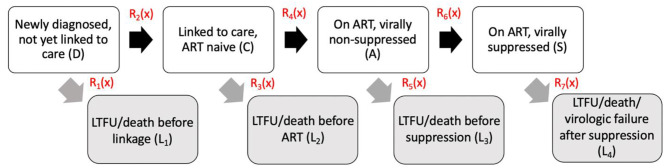
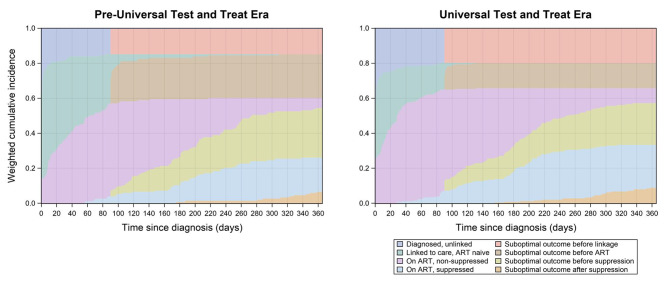
A total of 420 YLHIV were included. By day 365 following diagnosis, just 23% of individuals had no 90-or-more-day lapse in care and were virally suppressed. Those diagnosed in the UTT era spent less time as ART-naïve (mean difference=-19.3 days; 95% CI: -27.7, -10.9) and more time virally suppressed (mean difference = 17.7; 95% CI: 1.0, 34.4) compared to those diagnosed pre-UTT. Most individuals who were diagnosed in the UTT era and experienced a 90-or-more-day lapse in care disengaged between diagnosis and linkage to care or ART initiation and viral suppression.
Implementation of UTT yielded modest improvements in time spent on ART and virally suppressed among South African YLHIV- however, meeting UNAIDS' 95-95-95 targets remains a challenge. Retention in care and re-engagement interventions that can be implemented between diagnosis and linkage to care and between ART initiation and viral suppression (e.g., longitudinal counseling) may be particularly important to improving care outcomes among South African YLHIV in the UTT era.
对于普遍检测和治疗(UTT)政策对感染艾滋病毒的青年(YLHIV)的艾滋病毒护理结果的影响,我们知之甚少。此外,关于在最新治疗指南下,YLHIV 何时最容易脱离护理,相关信息也很少。纵向艾滋病毒护理连续统一体是一种未被充分利用的工具,可以全面了解人群级艾滋病毒护理轨迹,并用于比较不同群体的治疗结果。我们旨在探讨 UTT 政策对南非 YLHIV 纵向结局的影响,并确定在 UTT 时代重新使这一重点人群参与治疗的精确时机。
我们使用医疗记录数据,对 2015 年 8 月至 2018 年 12 月期间在南非九个医疗保健机构被诊断出感染艾滋病毒的 18-24 岁青年进行了回顾性队列研究。我们使用 Fine 和 Gray 亚分布比例风险模型,描述总体人群以及按诊断时的治疗时代分层的纵向护理连续统一体结局。我们估计了在每个阶段的个体比例,以及在诊断后第一年中每个阶段的受限平均时间。使用差异比较亚组估计值。
共纳入 420 名 YLHIV。在诊断后的第 365 天,只有 23%的人没有 90 天或以上的护理中断,并且病毒得到了抑制。与 UTT 前诊断的患者相比,在 UTT 时代诊断的患者处于初始抗逆转录病毒治疗(ART)前的时间更短(平均差异=-19.3 天;95%CI:-27.7,-10.9),病毒抑制的时间更长(平均差异=17.7;95%CI:1.0,34.4)。大多数在 UTT 时代诊断出患有 90 天或以上护理中断的患者,在诊断到与护理衔接或 ART 启动和病毒抑制之间脱离了护理。
在南非 YLHIV 中实施 UTT 使接受 ART 和病毒抑制的时间略有改善-然而,实现联合国艾滋病规划署的 95-95-95 目标仍然是一个挑战。保留护理和重新参与护理干预措施,可以在诊断到与护理衔接以及 ART 启动和病毒抑制之间实施(例如,纵向咨询),这可能对改善南非 YLHIV 在 UTT 时代的护理结果特别重要。