Department of Surgery and Anesthesiology, Ersta Hospital, Stockholm, Sweden.
Karolinska Institutet at Danderyd Hospital, Stockholm, Sweden.
JAMA Netw Open. 2023 Sep 5;6(9):e2332408. doi: 10.1001/jamanetworkopen.2023.32408.
A key objective in contemporary surgery is to reduce or eliminate the usage of opioids to minimize gastrointestinal adverse effects, fatigue, and long-term opioid dependency.
To evaluate the association of the implementation of a care bundle of 3 opioid-sparing interventions with the amount of opioids consumed postoperatively among patients undergoing major abdominal surgery and to examine the respective associations of the 3 components.
DESIGN, SETTING, AND PARTICIPANTS: This retrospective cohort study was performed at Ersta Hospital, an elective teaching hospital in Stockholm, Sweden. All patients undergoing major colorectal surgery between January 1, 2016, through December 31, 2019, were included. Data analysis was conducted from February 1, 2020, to May 30, 2022.
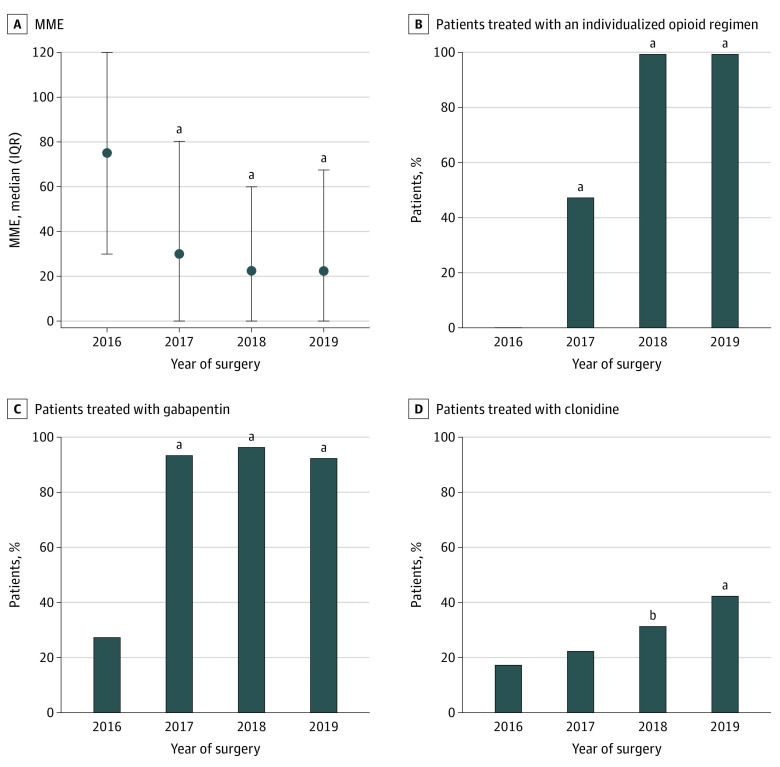
A care bundle consisting of an individualized opioid regimen, regular gabapentinoids, and clonidine as a rescue analgesic was gradually introduced early in the study period.
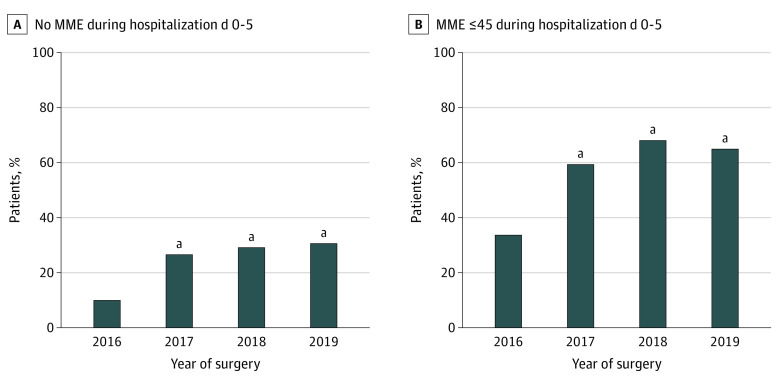
Amount of in-hospital administered intravenous and oral opioids on the day of surgery and the first 5 postoperative days (morphine milligram equivalents [MME]). The association between exposure and outcome was examined using multivariable linear regression.
Overall, 842 patients had major colorectal surgery in the study period (mean [SD] age, 64.6 [15.5] years; 421 [50%] men). Median (range) opioid usage decreased from 75 (0-796) MME in 2016 to 22 (0-362) MME in 2019 (P < .001), and the proportion of patients receiving 45 MME or less increased from 35% to 66% (P < .001). On multivariable analysis (F5, 836 = 57.5; P < .001), an individualized opioid strategy (β = -11.6; SE = 3.8; P = .003), the use of gabapentin (β = -39.1; SE = 4.5; P < .001), and increasing age (β = -1.0; SE = 0.11; P < .001) were associated with less opioid consumption, while the use of clonidine was associated with more opioid intake (β = 11.6; SE = 3.6; P = .001).
In this cohort study of 842 patients undergoing colorectal surgery, a care bundle consisting of an individualized opioid regimen, regular gabapentin, and clonidine as a rescue analgesic was found to be associated with a significant decrease in opioids consumed postoperatively. Regular gabapentin and an individualized opioid regimen were particularly strongly associated with this decrease and should be further evaluated as components of multimodal, opioid-free postoperative analgesia.
当代外科手术的一个主要目标是减少或消除阿片类药物的使用,以最大程度地减少胃肠道不良反应、疲劳和长期阿片类药物依赖。
评估实施 3 种阿片类药物节约干预措施的护理包与主要腹部手术后患者术后阿片类药物消耗量之间的关联,并分别检查这 3 个组成部分的各自关联。
设计、地点和参与者:这是一项在瑞典斯德哥尔摩的 Ersta 医院进行的回顾性队列研究。该研究纳入了 2016 年 1 月 1 日至 2019 年 12 月 31 日期间接受主要结直肠手术的所有患者。数据分析于 2020 年 2 月 1 日至 2022 年 5 月 30 日进行。
护理包由个体化阿片类药物方案、定期加巴喷丁类药物和可乐定作为解救镇痛剂组成,在研究早期逐渐引入。
手术当天和术后第 5 天(吗啡毫克当量 [MME])的静脉和口服阿片类药物的院内使用量。使用多变量线性回归检查暴露与结局之间的关联。
研究期间共有 842 名患者接受了结直肠手术(平均 [标准差] 年龄,64.6 [15.5] 岁;421 [50%] 为男性)。2016 年的中位(范围)阿片类药物使用量为 75(0-796)MME,降至 2019 年的 22(0-362)MME(P<0.001),接受 45 MME 或更少阿片类药物的患者比例从 35%增加到 66%(P<0.001)。多变量分析(F5,836=57.5;P<0.001)显示,个体化阿片类药物策略(β=-11.6;SE=3.8;P=0.003)、加巴喷丁的使用(β=-39.1;SE=4.5;P<0.001)和年龄增加(β=-1.0;SE=0.11;P<0.001)与阿片类药物消耗减少相关,而可乐定的使用与阿片类药物摄入增加相关(β=11.6;SE=3.6;P=0.001)。
在这项对 842 名接受结直肠手术的患者进行的队列研究中,发现由个体化阿片类药物方案、定期加巴喷丁和可乐定作为解救镇痛剂组成的护理包与术后阿片类药物消耗显著减少相关。定期加巴喷丁和个体化阿片类药物方案与这种减少特别密切相关,应作为多模式、无阿片类药物术后镇痛的组成部分进一步评估。