Anaesthesia, Critical Care & Peri-operative Medicine Research Group, University of Glasgow, Glasgow, UK.
Department of Anaesthesia, Golden National Jubilee Hospital, Clydebank, UK.
BMJ Open. 2023 Sep 6;13(9):e074687. doi: 10.1136/bmjopen-2023-074687.
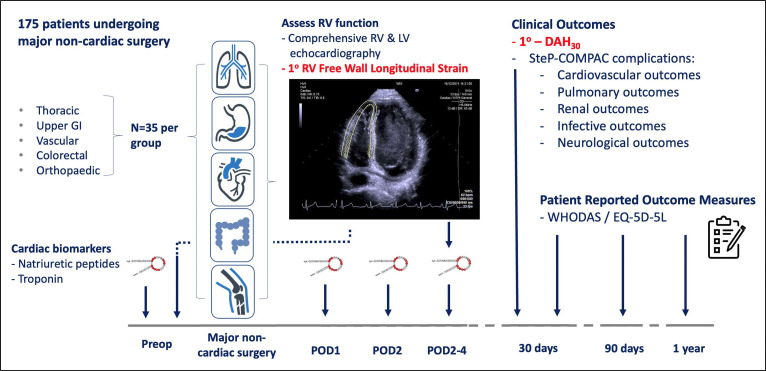
Perioperative myocardial injury evidenced by elevated cardiac biomarkers (both natriuretic peptides and troponin) is common after major non-cardiac surgery. However, it is unclear if the rise in cardiac biomarkers represents global or more localised cardiac injury. We have previously shown isolated right ventricular (RV) dysfunction in patients following lung resection surgery, with no change in left ventricular (LV) function. Given that perioperative RV dysfunction (RVD) can manifest insidiously, we hypothesise there may be a substantial burden of covert yet clinically important perioperative RVD in other major non-cardiac surgical groups. The Incidence, impact and Mechanisms of Perioperative Right VEntricular dysfunction (IMPRoVE) study has been designed to address this knowledge gap.
A multicentre prospective observational cohort study across four centres in the West of Scotland and London. One hundred and seventy-five patients will be recruited from five surgical specialties: thoracic, upper gastrointestinal, vascular, colorectal and orthopaedic surgery (35 patients from each group). All patients will undergo preoperative and postoperative (day 2-4) echocardiography, with contemporaneous cardiac biomarker testing. Ten patients from each surgical specialty (50 patients in total) will undergo T1-cardiovascular magnetic resonance (CMR) imaging preoperatively and postoperatively. The coprimary outcomes are the incidence of perioperative RVD (diagnosed by RV speckle tracking echocardiography) and the effect that RVD has on days alive and at home at 30 days postoperatively. Secondary outcomes include LV dysfunction and clinical outcomes informed by Standardised Endpoints in Perioperative Medicine consensus definitions. T1 CMR will be used to investigate for imaging correlates of myocardial inflammation as a possible mechanism driving perioperative RVD.
Approval was gained from Oxford C Research Ethics Committee (REC reference 22/SC/0442). Findings will be disseminated by various methods including social media, international presentations and publication in peer-reviewed journals.
NCT05827315.
在非心脏大手术后,升高的心脏生物标志物(包括利钠肽和肌钙蛋白)可证实围手术期心肌损伤。然而,升高的心脏生物标志物是否代表了整体或更局部的心肌损伤尚不清楚。我们之前已经证明,在肺切除术后患者中存在孤立的右心室(RV)功能障碍,而左心室(LV)功能没有变化。鉴于围手术期 RV 功能障碍(RVD)可能隐匿性出现,我们假设在其他主要非心脏手术组中可能存在大量隐匿但临床上重要的围手术期 RVD。为了填补这一知识空白,我们设计了“围手术期右心室功能障碍的发生率、影响和机制(IMPRoVE)”研究。
这是一项横跨苏格兰西部和伦敦的四个中心的多中心前瞻性观察队列研究。将从五个外科专业(胸外科、上消化道外科、血管外科、结直肠外科和矫形外科)中招募 175 名患者(每组 35 名患者)。所有患者将在术前和术后(第 2-4 天)进行超声心动图检查,并同时进行心脏生物标志物检测。每个外科专业将有 10 名患者(共 50 名患者)进行术前和术后 T1 心血管磁共振(CMR)成像。主要结局是围手术期 RVD 的发生率(通过 RV 斑点追踪超声心动图诊断)和 RVD 对术后 30 天存活和在家天数的影响。次要结局包括 LV 功能障碍和由围手术期医学标准化终点共识定义的临床结局。T1 CMR 将用于研究心肌炎症的影像学相关性,作为导致围手术期 RVD 的可能机制。
牛津 C 研究伦理委员会(REC 参考号 22/SC/0442)已批准。研究结果将通过各种方法传播,包括社交媒体、国际演讲和在同行评议期刊上发表。
NCT05827315。