From the Vanderbilt University School of Medicine.
Vanderbilt University.
Anesth Analg. 2023 Nov 1;137(5):996-1006. doi: 10.1213/ANE.0000000000006600. Epub 2023 Oct 20.
Renal ischemia and reperfusion (IR) contribute to perioperative acute kidney injury, and oxygen is a key regulator of this process. We hypothesized that oxygen administration during surgery and renal IR would impact postoperative kidney function and injury in mice.
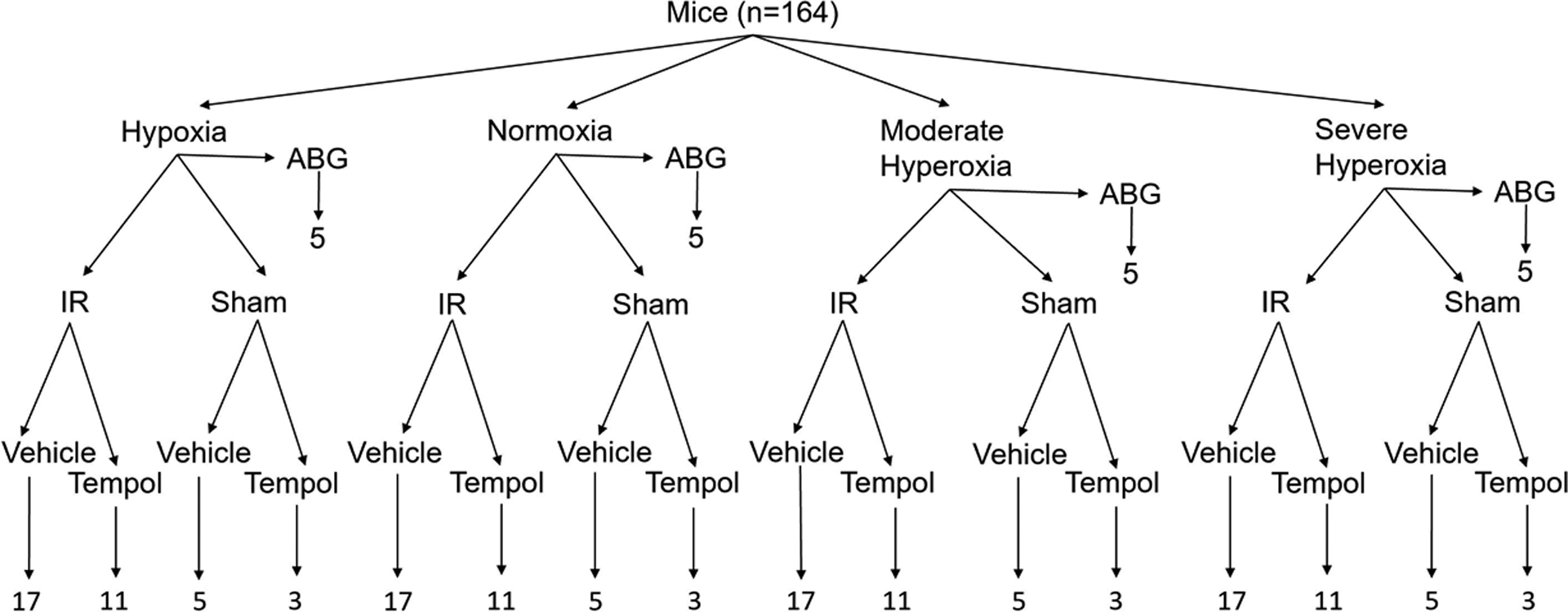
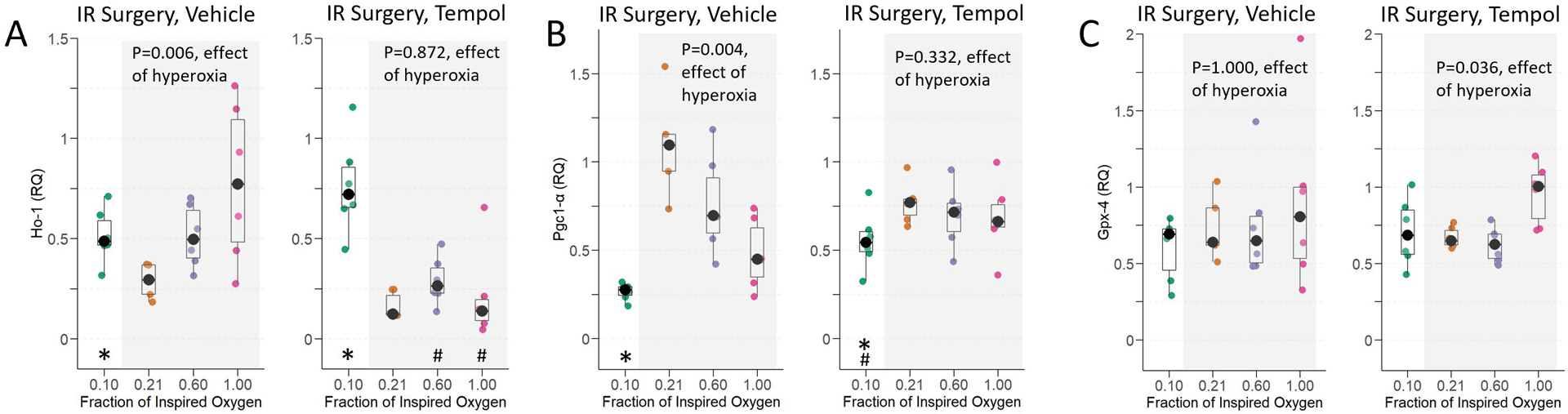
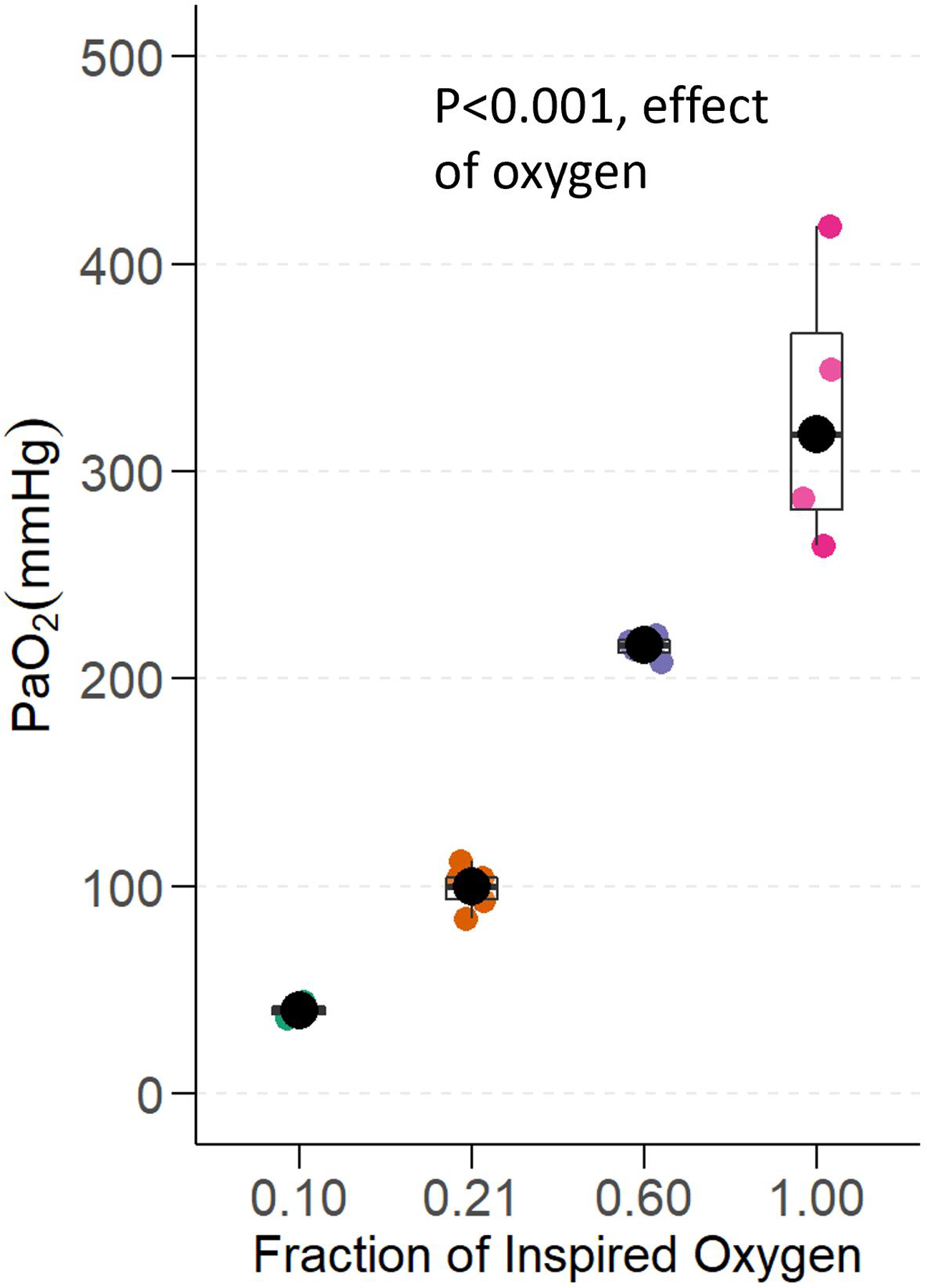
Mice were anesthetized, intubated, and mechanically ventilated with a fraction of inspired oxygen (F io2 ) 0.10 (hypoxia), 0.21 (normoxia), 0.60 (moderate hyperoxia), or 1.00 (severe hyperoxia) during 67 minutes of renal IR or sham IR surgery. Additional mice were treated before IR or sham IR surgery with 50 mg/kg tempol, a superoxide scavenger. At 24 hours, mice were sacrificed, and blood and kidney collected. We assessed and compared kidney function and injury across groups by measuring blood urea nitrogen (BUN, primary end point), renal histological injury, renal expression of neutrophil gelatinase-associated lipocalin (NGAL), and renal heme oxygenase 1 ( Ho-1 ), peroxisome proliferator-activated receptor gamma coactivator 1-α ( Pgc1-α ), and glutathione peroxidase 4 ( Gpx-4 ) transcripts, to explore potential mechanisms of any effect of oxygen.
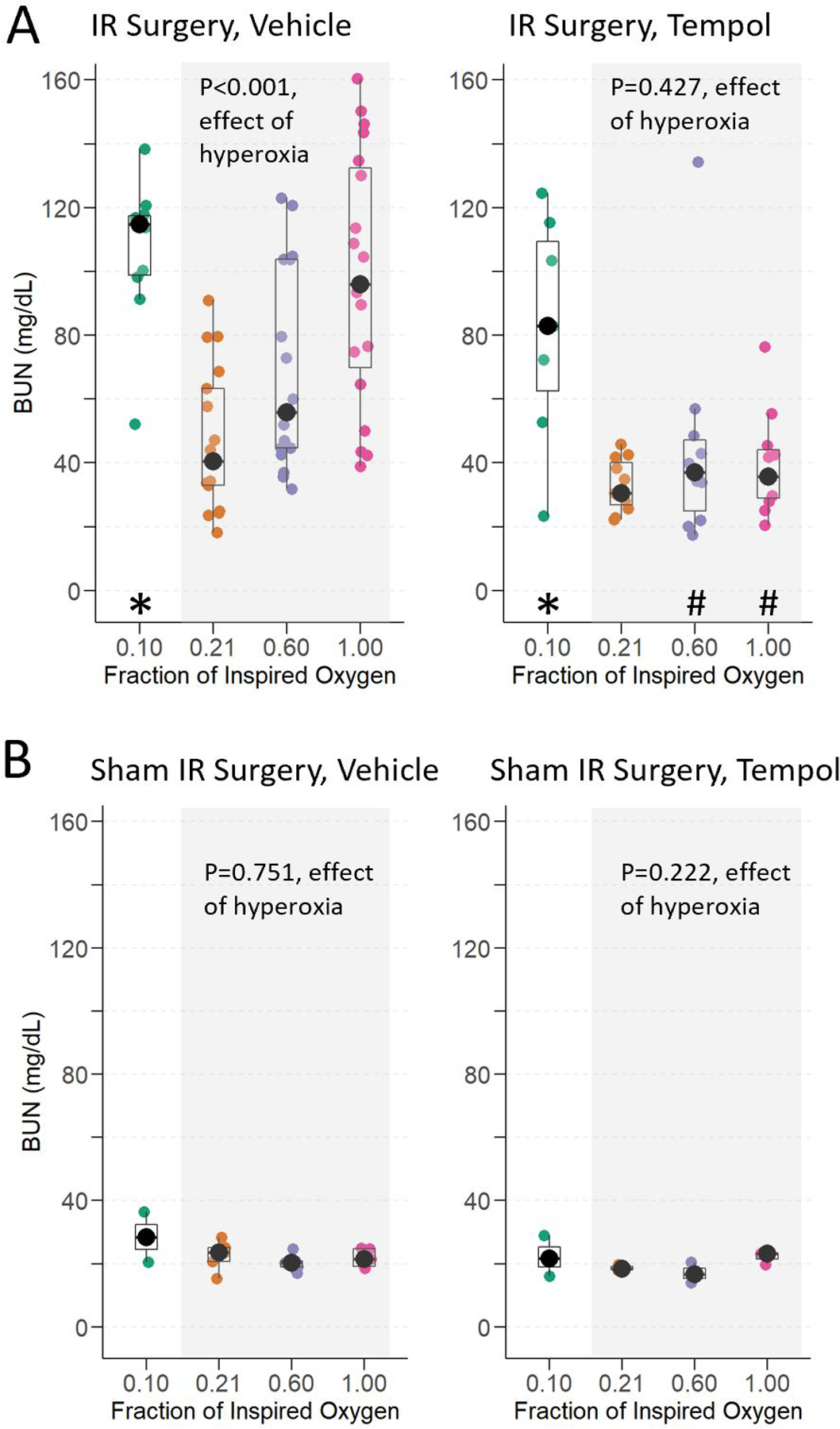
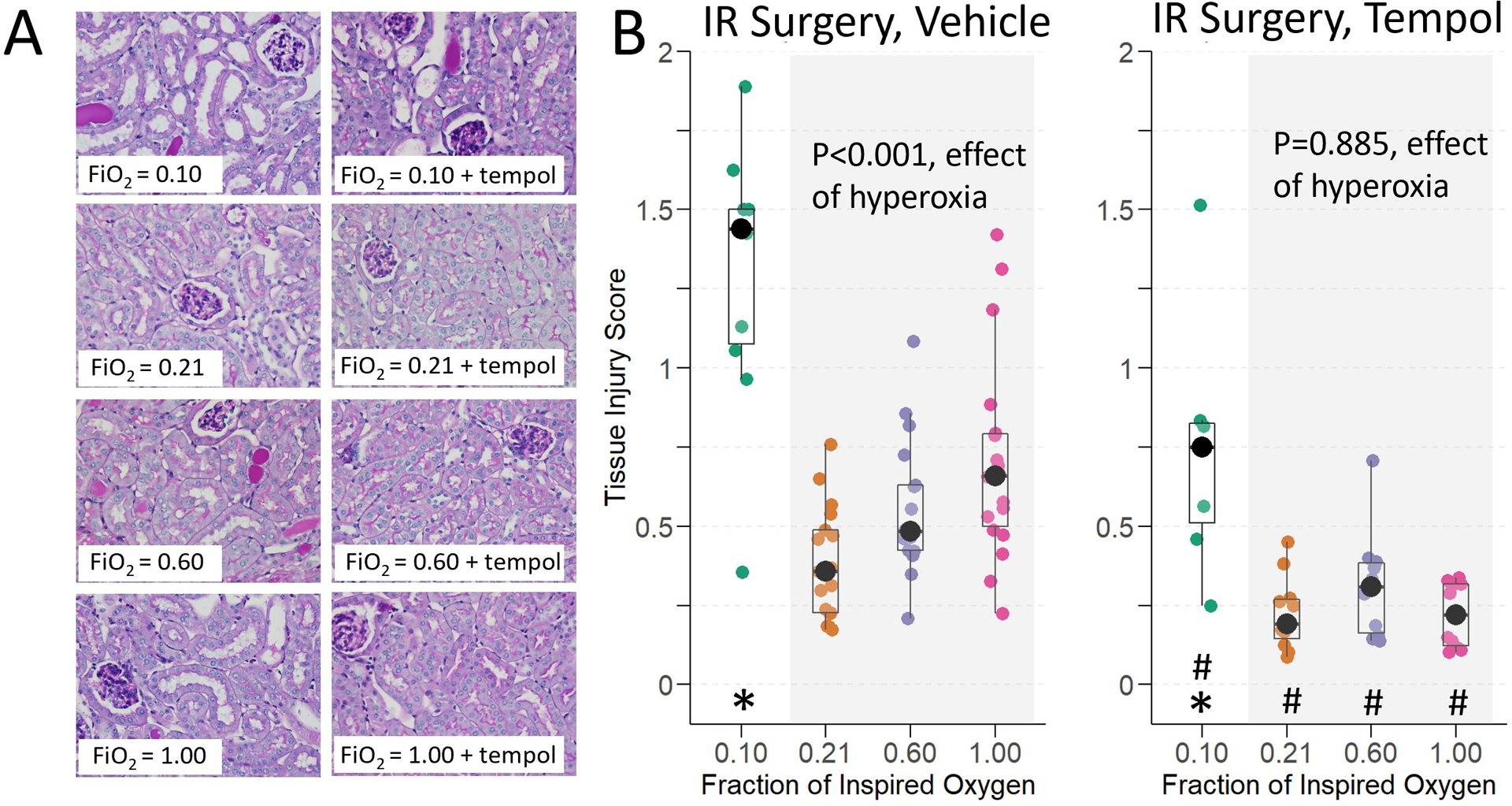
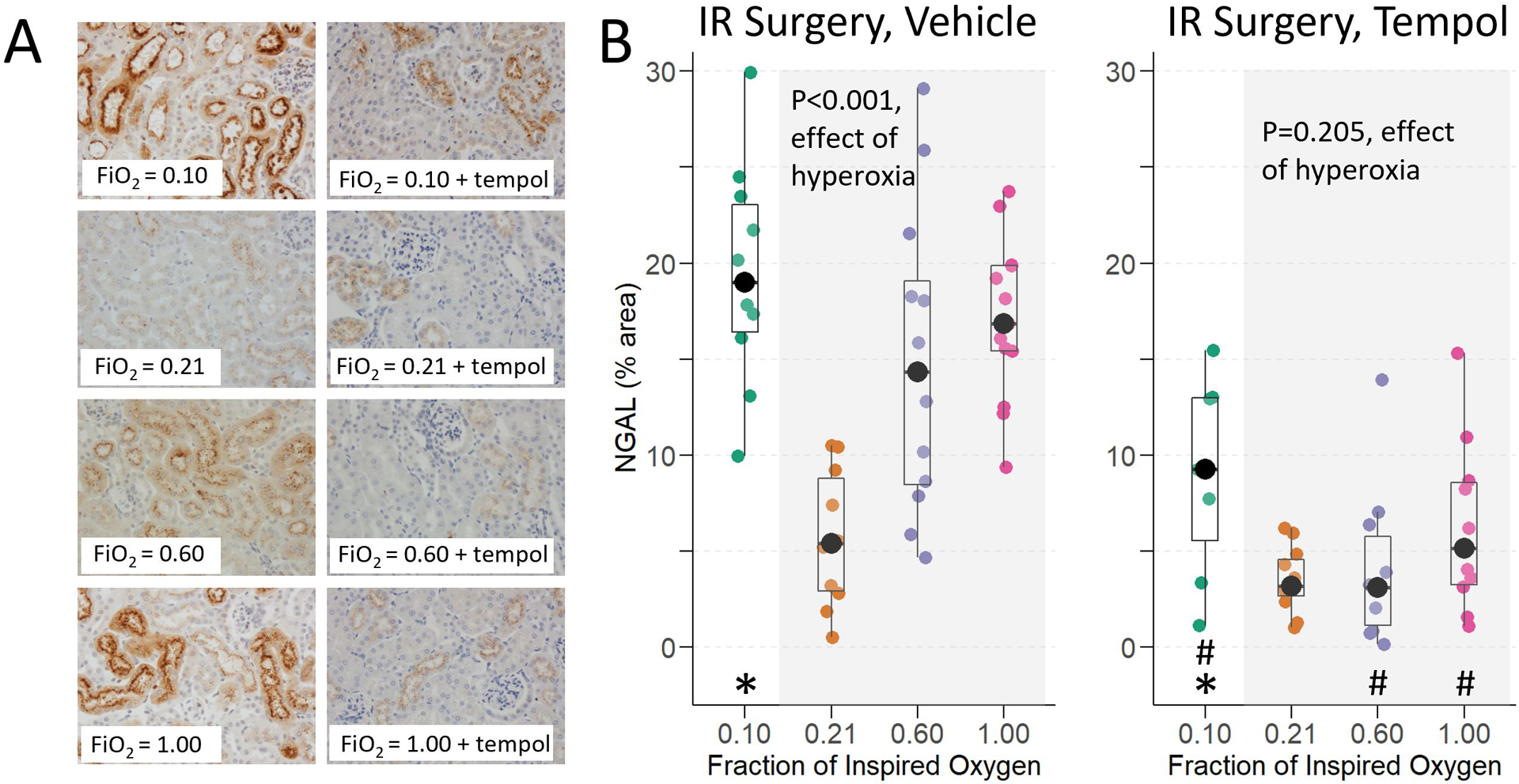
Hyperoxia and hypoxia during renal IR surgery decreased renal function and increased kidney injury compared to normoxia. Baseline median (interquartile range) BUN was 22.2 mg/dL (18.4-26.0), and 24 hours after IR surgery, BUN was 17.5 mg/dL (95% confidence interval [CI], 1.3-38.4; P = .034) higher in moderate hyperoxia-treated animals, 51.8 mg/dL (95% CI, 24.9-74.8; P < .001) higher in severe hyperoxia-treated animals, and 64.9 mg/dL (95% CI, 41.2-80.3; P < .001) higher in hypoxia-treated animals compared to animals treated with normoxia ( P < .001, overall effect of hyperoxia). Hyperoxia-induced injury, but not hypoxia-induced injury, was attenuated by pretreatment with tempol. Histological injury scores, renal NGAL staining, and renal transcription of Ho-1 and suppression of Pgc1- α followed the same pattern as BUN, in relation to the effects of oxygen treatment.
In this controlled preclinical study of oxygen treatment during renal IR surgery, hyperoxia and hypoxia impaired renal function, increased renal injury, and impacted expression of genes that affect mitochondrial biogenesis and antioxidant response. These results might have implications for patients during surgery when high concentrations of oxygen are frequently administered, especially in cases involving renal IR.
肾缺血再灌注(IR)导致围手术期急性肾损伤,而氧是此过程的关键调节剂。我们假设手术期间和肾 IR 期间的氧给与会影响小鼠的术后肾功能和损伤。
在肾 IR 或假手术期间,将小鼠麻醉、插管并机械通气,吸入氧分数(Fio2)为 0.10(缺氧)、0.21(常氧)、0.60(中度高氧)或 1.00(重度高氧),持续 67 分钟。在 IR 或假手术之前,用 50mg/kg 特布他林(超氧化物清除剂)治疗其他小鼠。24 小时后,处死小鼠并收集血液和肾脏。通过测量血尿素氮(BUN,主要终点)、肾脏组织学损伤、肾脏中性粒细胞明胶酶相关脂质运载蛋白(NGAL)的表达以及肾脏血红素加氧酶 1(Ho-1)、过氧化物酶体增殖物激活受体 γ共激活因子 1-α(Pgc1-α)和谷胱甘肽过氧化物酶 4(Gpx-4)转录物,评估和比较各组的肾功能和损伤,以探索氧的任何作用的潜在机制。
与常氧相比,肾 IR 手术期间的高氧和低氧降低了肾功能并增加了肾脏损伤。基线中位数(四分位距)BUN 为 22.2mg/dL(18.4-26.0),IR 手术后 24 小时,中度高氧处理动物的 BUN 升高 17.5mg/dL(95%置信区间 [CI],1.3-38.4;P=.034),重度高氧处理动物升高 51.8mg/dL(95%CI,24.9-74.8;P<.001),低氧处理动物升高 64.9mg/dL(95%CI,41.2-80.3;P<.001),与常氧处理动物相比(P<.001,高氧的总体影响)。特布他林预处理可减轻高氧诱导的损伤,但不能减轻低氧诱导的损伤。组织学损伤评分、肾脏 NGAL 染色以及 Ho-1 和 Pgc1-α 的肾转录均与氧处理的影响一致,与 BUN 的结果相似。
在这项关于肾 IR 手术期间氧治疗的对照性临床前研究中,高氧和低氧降低了肾功能,增加了肾脏损伤,并影响了影响线粒体生物发生和抗氧化反应的基因的表达。这些结果可能对手术期间经常给予高浓度氧气的患者具有重要意义,尤其是在涉及肾 IR 的情况下。