Andreacchi Alessandra T, Smith Brendan T, Rehm Jürgen, Crépault Jean-François, Sherk Adam, Hobin Erin
Health Promotion, Chronic Disease and Injury Prevention, Public Health Ontario, Toronto, ON, Canada.
Dalla Lana School of Public Health, University of Toronto, Toronto, ON, Canada.
Prev Med Rep. 2023 Aug 25;35:102388. doi: 10.1016/j.pmedr.2023.102388. eCollection 2023 Oct.
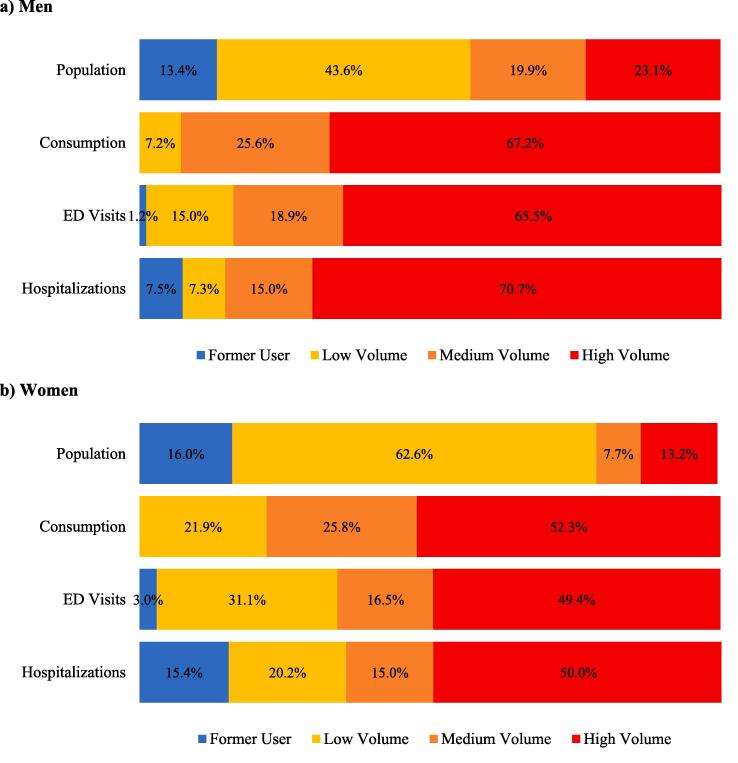
Recent evidence suggests there may be no safe level of alcohol use as even low levels are associated with increased risk for harm. However, the magnitude of the population-level health burden from lower levels of alcohol use is poorly understood. The objective was to estimate the distribution of alcohol-attributable healthcare encounters (emergency department (ED) visits and hospitalizations) across the population of alcohol users aged 15+ in Ontario, Canada. Using the International Model of Alcohol Harms and Policies (InterMAHP) tool, wholly and partially alcohol-attributable healthcare encounters were estimated across alcohol users: (1) former (no past-year use); (2) low volume (≤67.3 g ethanol/week); (3) medium volume (>67.3-134.5 g ethanol/week for women and >67.3-201.8 g ethanol/week for men); and (4) high volume (>134.5 g ethanol/week for women and >201.8 g ethanol/week for men). The alcohol-attributable healthcare burden was distributed across the population of alcohol users. A small population of high volume users (23% of men, 13% of women) were estimated to have contributed to the greatest proportion of alcohol-attributable healthcare encounters, particularly among men (men: 65% of ED visits and 71% of hospitalizations, women: 49% of ED visits and 50% of hospitalizations). The 71% of women low and medium volumes users were estimated to have contributed to a substantial proportion of alcohol-attributable healthcare encounters (47% of ED visits and 34% of hospitalizations). Findings provide support for universal alcohol policies (i.e., delivered to the entire population) for reducing population-level alcohol-attributable harm in addition to targeted policies for high-risk users.
近期证据表明,饮酒可能不存在安全剂量,因为即使少量饮酒也会增加伤害风险。然而,人们对低水平饮酒给人群健康带来的负担程度知之甚少。目的是估计加拿大安大略省15岁及以上饮酒人群中酒精所致医疗接触(急诊就诊和住院)的分布情况。使用国际酒精危害与政策模型(InterMAHP)工具,对饮酒者中完全和部分由酒精所致的医疗接触进行了估计:(1)既往饮酒者(过去一年未饮酒);(2)低饮酒量者(≤67.3克乙醇/周);(3)中等饮酒量者(女性>67.3 - 134.5克乙醇/周,男性>67.3 - 201.8克乙醇/周);以及(4)高饮酒量者(女性>134.5克乙醇/周,男性>201.8克乙醇/周)。酒精所致的医疗负担在饮酒人群中进行了分布。据估计,一小部分高饮酒量使用者(23%的男性,13%的女性)导致了酒精所致医疗接触的最大比例,尤其是在男性中(男性:65%的急诊就诊和71%的住院,女性:49%的急诊就诊和50%的住院)。据估计,71%的低饮酒量和中等饮酒量女性使用者导致了相当比例的酒精所致医疗接触(47%的急诊就诊和34%的住院)。研究结果支持除针对高危使用者的针对性政策外,还应实施普遍性酒精政策(即针对全体人群)以减少人群层面酒精所致的伤害。