Zhong Xian, Long Haiyi, Chen Lili, Xie Yuhua, Shi Yifan, Peng Jianyun, Zheng Ruiying, Su Liya, Duan Yu, Xie Xiaoyan, Lin Manxia
Department of Ultrasound, The First Affiliated Hospital of Sun Yat-Sen University, 58 Zhongshan Second Road, Guangzhou, 510080, China.
Department of Pathology, The First Affiliated Hospital of Sun Yat-Sen University, 58 Zhongshan Second Road, Guangzhou, 510080, China.
Insights Imaging. 2023 Sep 12;14(1):147. doi: 10.1186/s13244-023-01505-7.
To explore the pathologic basis and prognostic value of tumor and liver stiffness measured pre-operatively by two-dimensional shear wave elastography (2D-SWE) in hepatitis B virus (HBV)-related hepatocellular carcinoma (HCC) patients who undergo hepatic resection.
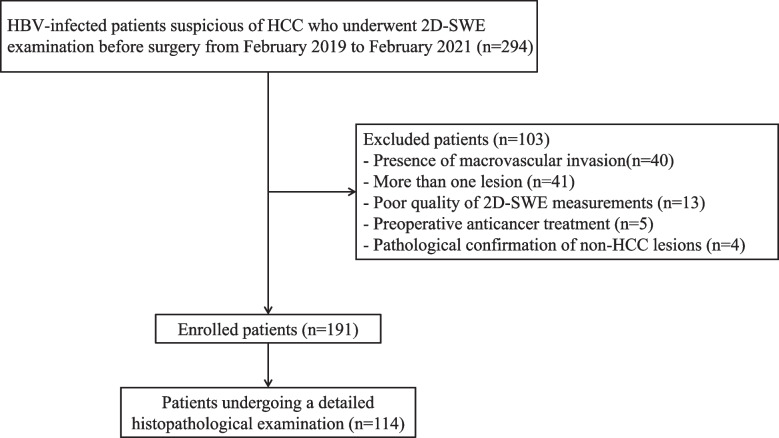
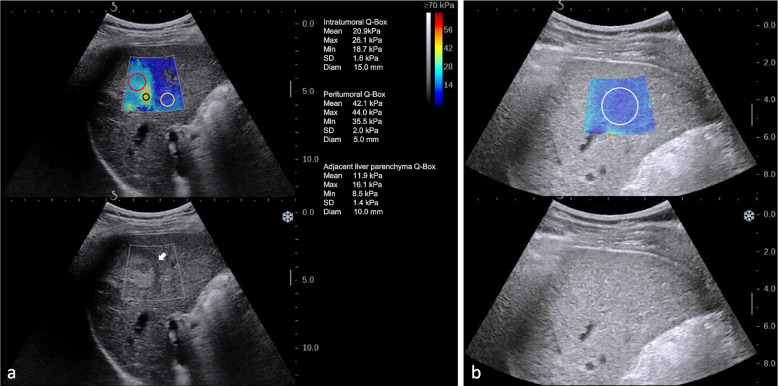
A total of 191 HBV-infected patients with solitary resectable HCC were prospectively enrolled. The stiffness of intratumoral tissue, peritumoral tissue, adjacent liver tissue, and distant liver tissue was evaluated by 2D-SWE. The correlations between stiffness and pathological characteristics were analyzed in 114 patients. The predictive value of stiffness for recurrence-free survival (RFS) was evaluated, and Cutoff Finder was used for determining optimal cut-off stiffness values. Cox proportional hazards analysis was used to identify independent predictors of RFS.
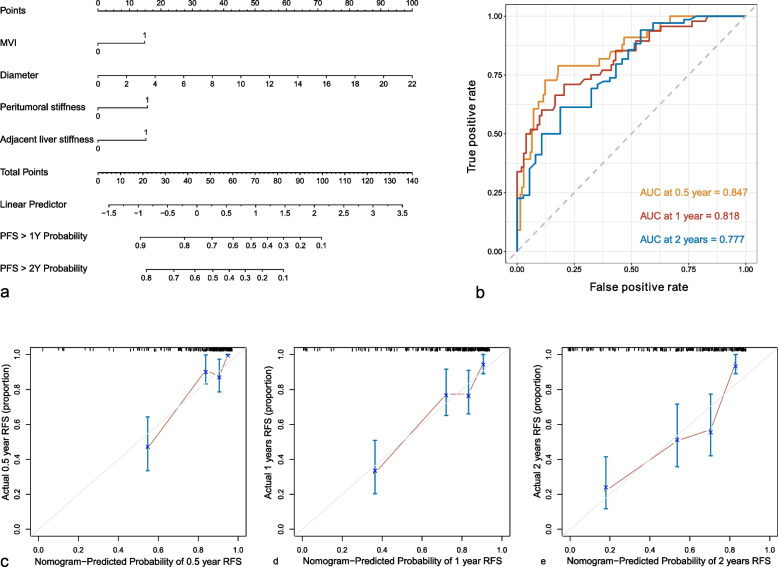
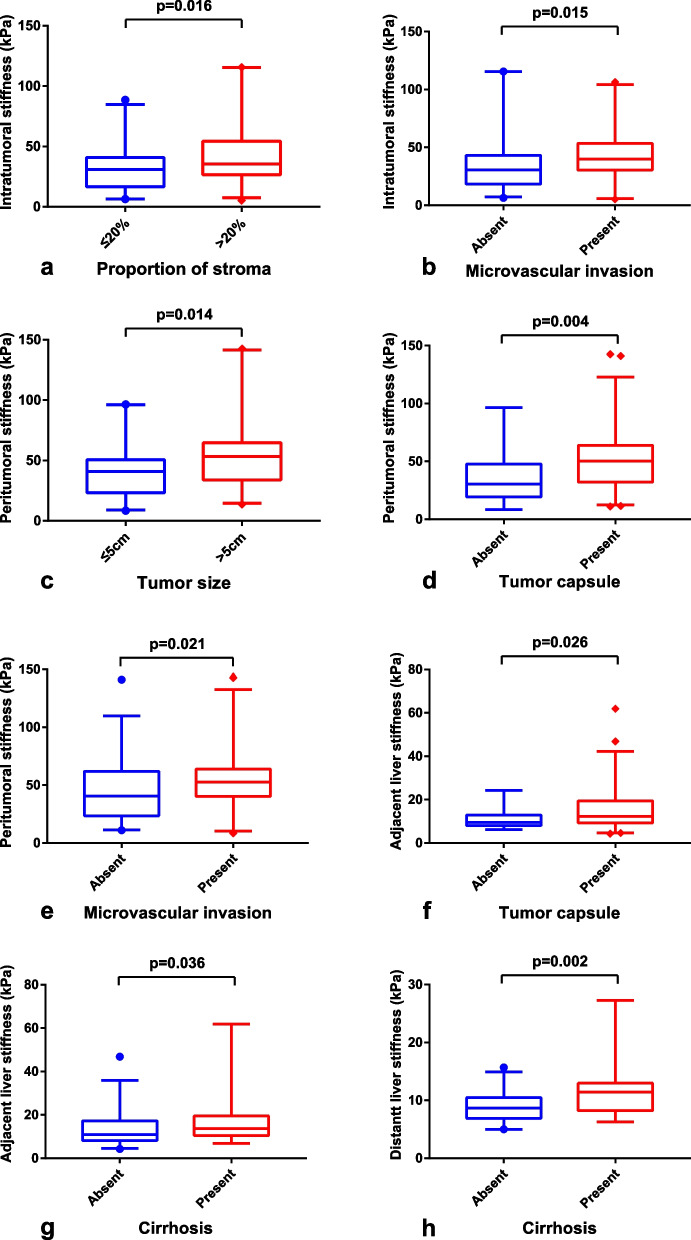
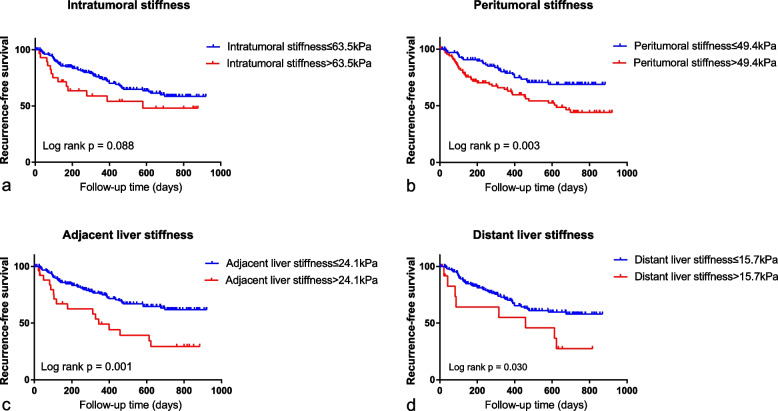
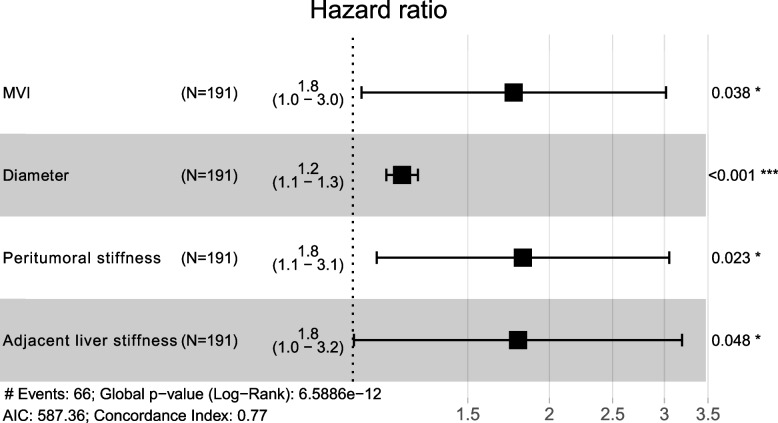
Pathologically, intratumoral stiffness was associated with stroma proportion and microvascular invasion (MVI) while peritumoral stiffness was associated with tumor size, capsule, and MVI. Adjacent liver stiffness was correlated with capsule and liver fibrosis stage while distant liver stiffness was correlated with liver fibrosis stage. Peritumoral stiffness, adjacent liver stiffness, and distant liver stiffness were all correlated to RFS (all p < 0.05). Higher peritumoral stiffness (> 49.4 kPa) (HR = 1.822, p = 0.023) and higher adjacent liver stiffness (> 24.1 kPa) (HR = 1.792, p = 0.048) were significant independent predictors of worse RFS, along with tumor size and MVI. The nomogram based on these variables showed a C-index of 0.77 for RFS prediction.
Stiffness measured by 2D-SWE could be a tumor microenvironment and tumor invasiveness biomarker. Peritumoral stiffness and adjacent liver stiffness showed important values in predicting tumor recurrence after curative resection in HBV-related HCC.
Tumor and liver stiffness measured by two-dimensional shear wave elastography serve as imaging biomarkers for predicting hepatocellular carcinoma recurrence, reflecting biological behavior and tumor microenvironment.
• Stiffness measured by two-dimensional shear wave elastography is a useful biomarker of tumor microenvironment and invasiveness. • Higher stiffness indicated more aggressive behavior of hepatocellular carcinoma. • The study showed the prognostic value of peritumoral stiffness and adjacent liver stiffness for recurrence-free survival. • The nomogram integrating peritumoral stiffness, adjacent liver stiffness, tumor size, and microvascular invasion showed a C-index of 0.77.
探讨二维剪切波弹性成像(2D-SWE)术前测量的肿瘤及肝脏硬度在接受肝切除的乙型肝炎病毒(HBV)相关肝细胞癌(HCC)患者中的病理基础及预后价值。
前瞻性纳入191例HBV感染的孤立性可切除HCC患者。采用2D-SWE评估瘤内组织、瘤周组织、邻近肝组织及远处肝组织的硬度。对114例患者分析硬度与病理特征之间的相关性。评估硬度对无复发生存期(RFS)的预测价值,并使用Cutoff Finder确定最佳临界硬度值。采用Cox比例风险分析确定RFS的独立预测因素。
病理上,瘤内硬度与间质比例和微血管侵犯(MVI)相关,而瘤周硬度与肿瘤大小、包膜及MVI相关。邻近肝硬度与包膜及肝纤维化分期相关,远处肝硬度与肝纤维化分期相关。瘤周硬度、邻近肝硬度及远处肝硬度均与RFS相关(均p<0.05)。较高的瘤周硬度(>49.4 kPa)(HR=1.822,p=0.023)和较高的邻近肝硬度(>24.1 kPa)(HR=1.792,p=0.048)是RFS较差的显著独立预测因素,同时还有肿瘤大小和MVI。基于这些变量的列线图显示RFS预测的C指数为0.77。
2D-SWE测量的硬度可能是一种肿瘤微环境及肿瘤侵袭性生物标志物。瘤周硬度和邻近肝硬度在预测HBV相关HCC根治性切除术后肿瘤复发方面显示出重要价值。
二维剪切波弹性成像测量的肿瘤及肝脏硬度作为预测肝细胞癌复发的影像生物标志物,反映生物学行为和肿瘤微环境。
•二维剪切波弹性成像测量的硬度是肿瘤微环境及侵袭性的有用生物标志物。•较高的硬度表明肝细胞癌的侵袭性更强。•该研究显示了瘤周硬度和邻近肝硬度对无复发生存期的预后价值。•整合瘤周硬度、邻近肝硬度、肿瘤大小和微血管侵犯的列线图显示C指数为0.77。