Department of Perioperative Medicine and Intensive Care, Karolinska University Hospital, Stockholm, Sweden.
Section of Perioperative Medicine and Intensive Care, Department of Physiology and Pharmacology, Karolinska Institutet, Stockholm, Sweden.
Neurocrit Care. 2024 Apr;40(2):391-394. doi: 10.1007/s12028-023-01829-8. Epub 2023 Sep 11.
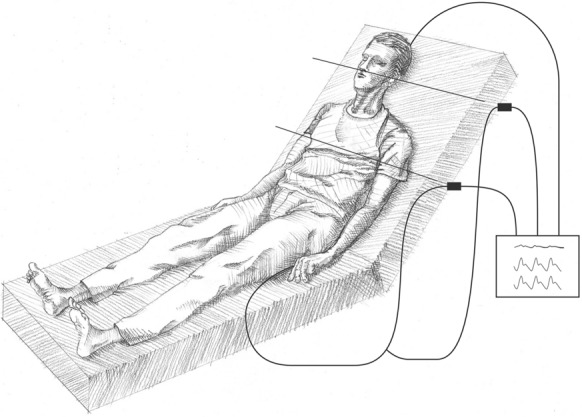
Intracranial pressure is routinely monitored in most intensive care units caring for patients with severe neurological insults and, together with continuous arterial blood pressure measurement, allows for monitoring of cerebral perfusion pressure (CPP). CPP is the driving pressure of blood flow to the brain and is used to guide therapy. However, there is considerable inconsistency in the literature regarding how CPP is technically measured and, more specifically, the appropriate placement of the arterial pressure transducer. Depending on patient positioning and where the arterial pressure transducer is placed, the mean arterial pressure used for CPP calculation can vary widely by up to 15 mm Hg, which is greater than the acceptable variation in target ranges used clinically. Physiologically, the arterial pressure transducer should be placed at the level of the foramen of Monro for CPP measurement, but it is commonly set at the level of the right atrium for systematic measurement. Mean arterial pressure measurement at the level of the right atrium can lead to overestimation and potentially critically low actual CPP levels when the head is elevated, and measurement at the level of the foramen of Monro will underestimate systemic pressures, increasing the risk of excessive and unnecessary use of vasopressors and fluid. At the Karolinska University Hospital neurointensive care unit, we have used a split dual-transducer system, measuring arterial pressure both at the level of the foramen of Monro and at the level of the right atrium from a single arterial source. In doing so, we work with constants and can monitor and target optimum arterial pressures to better secure perfusion to all organs, with potentially less risk of cerebral ischemia or overuse of vasopressors and fluids, which may affect outcome.
颅内压在大多数重症监护病房中都会进行常规监测,这些病房主要收治有严重神经损伤的患者。颅内压与连续动脉血压测量相结合,可以监测脑灌注压(CPP)。CPP 是大脑血流的驱动力,用于指导治疗。然而,关于 CPP 的技术测量方法,以及更具体地说,动脉压力换能器的适当放置位置,文献中存在相当大的不一致。根据患者的体位和动脉压力换能器的放置位置,用于 CPP 计算的平均动脉压可能会有很大差异,最高可达 15mmHg,这超过了临床上可接受的目标范围的变化。从生理学角度来看,CPP 测量时动脉压力换能器应置于孟氏孔水平,但为了进行系统测量,通常将其置于右心房水平。当头部抬高时,右心房水平的平均动脉压测量可能会导致高估,实际 CPP 水平可能极低,甚至危及生命;而孟氏孔水平的测量会低估系统性血压,增加过度和不必要使用血管加压药和液体的风险。在卡罗林斯卡大学医院神经重症监护病房,我们使用了一种分体式双传感器系统,从单个动脉源同时测量孟氏孔水平和右心房水平的动脉压。通过这种方式,我们使用常数工作,可以监测和针对最佳动脉压,以更好地确保所有器官的灌注,潜在地降低脑缺血或血管加压药和液体过度使用的风险,这可能会影响结果。