Dimov Diyan, Brainman Daniel, Berger Björn, Coras Roland, Grote Alexander, Simon Matthias
Department of Neurosurgery, Evangelisches Klinikum Bethel, Universitätsklinikum OWL, Bielefeld, Germany.
Department of Neuroradiology, Evangelisches Klinikum Bethel, Universitätsklinikum OWL, Bielefeld, Germany.
J Neurooncol. 2023 Sep;164(2):447-459. doi: 10.1007/s11060-023-04410-7. Epub 2023 Sep 12.
Multifocal/multicentric glioblastomas (mGBM) account for up to 20% of all newly diagnosed glioblastomas. The present study investigates the impact of cytoreductive surgery on survival and functional outcomes in patients with mGBM.
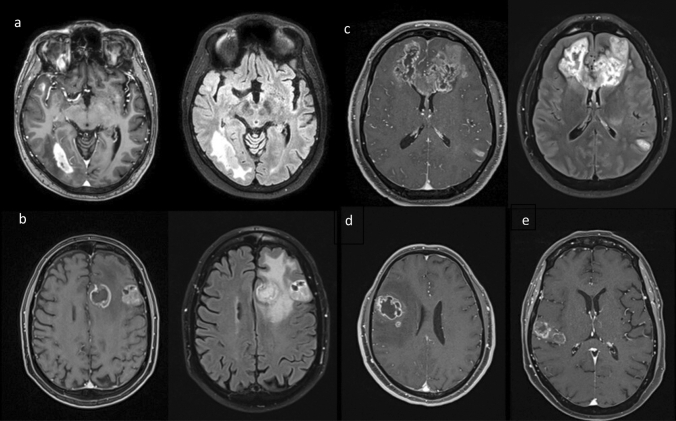
We retrospectively reviewed clinical and imaging data of 71 patients with newly diagnosed primary (IDH1 wildtype) mGBM who underwent operative treatment in 2015-2020 at the authors' institution. Multicentric/multifocal growth was defined by the presence of ≥ 2 contrast enhancing lesions ≥ 1 cm apart from each other.
36 (50.7%) patients had a resection and 35 (49.3%) a biopsy procedure. MGMT status, age, preoperative KPI and NANO scores as well as the postoperative KPI and NANO scores did not differ significantly between resected and biopsied cases. Median overall survival was 6.4 months and varied significantly with the extent of resection (complete resection of contrast enhancing tumor: 13.6, STR: 6.4, biopsy: 3.4 months; P = 0.043). 21 (58.3%) of resected vs. only 12 (34.3%) of biopsied cases had radiochemotherapy (p = 0.022). Multivariate analysis revealed chemo- and radiotherapy and also (albeit with smaller hazard ratios) extent of resection (resection vs. biopsy) and multicentric growth as independent predictors of patient survival. Involvement of eleoquent brain regions, as well as neurodeficit rates and functional outcomes did not vary significantly between the biopsy and the resection cohorts.
Resective surgery in mGBM is associated with better survival. This benefit seems to relate prominently to an increased number of patients being able to tolerate effective adjuvant therapies after tumor resections. In addition, cytoreductive surgery may have a survival impact per se.
多灶性/多中心性胶质母细胞瘤(mGBM)占所有新诊断胶质母细胞瘤的比例高达20%。本研究调查了减瘤手术对mGBM患者生存及功能结局的影响。
我们回顾性分析了2015年至2020年在作者所在机构接受手术治疗的71例新诊断的原发性(异柠檬酸脱氢酶1野生型)mGBM患者的临床和影像数据。多中心/多灶性生长定义为存在≥2个相互距离≥1 cm的强化病灶。
36例(50.7%)患者接受了切除术,35例(49.3%)患者接受了活检。切除组和活检组之间的O6-甲基鸟嘌呤-DNA甲基转移酶(MGMT)状态、年龄、术前KPI和NANO评分以及术后KPI和NANO评分无显著差异。中位总生存期为6.4个月,且随切除范围有显著差异(强化肿瘤完全切除:13.6个月,次全切除:6.4个月,活检:3.4个月;P = 0.043)。切除组21例(58.3%)接受了放化疗,而活检组仅12例(34.3%)接受了放化疗(p = 0.022)。多因素分析显示,化疗、放疗以及(尽管风险比更小)切除范围(切除与活检)和多中心生长是患者生存的独立预测因素。活检组和切除组之间,功能区脑区受累情况、神经功能缺损率及功能结局无显著差异。
mGBM的切除手术与更好的生存相关。这种益处似乎主要与肿瘤切除后能够耐受有效辅助治疗的患者数量增加有关。此外,减瘤手术本身可能对生存有影响。