Department of Hepatobiliary Surgery, Mengchao Hepatobiliary Hospital of Fujian Medical University, No. 312, Xihong Road, Fuzhou, Fujian, 350025, PR China.
Department of Hepatobiliary Surgery, Clinical Oncology School of Fujian Medical University, No. 420, Fuma Road, Fuzhou, Fujian, 350014, PR China.
BMC Cancer. 2023 Sep 11;23(1):850. doi: 10.1186/s12885-023-11341-z.
Radical resection is still the most cost-effectiveness curative strategy for intrahepatic cholangiocarcinoma (ICC), but it remains controversial on the survival benefit of anatomic resection (AR). In this study, we sought to compare the oncologic outcomes between AR versus non-AR (NAR) as the primary treatment for early-stage ICC patients.
Data of ICC patients who underwent hepatectomy and staged at AJCC I were retrospectively collected from 12 hepatobiliary centers in China between Dec 2012 and Dec 2015. Propensity score matching (PSM) and stabilized inverse probability of treatment weighting (IPTW) analysis were performed to minimize the effect of potential confounders, and the perioperative and long-term outcomes between AR and NAR groups were compared.
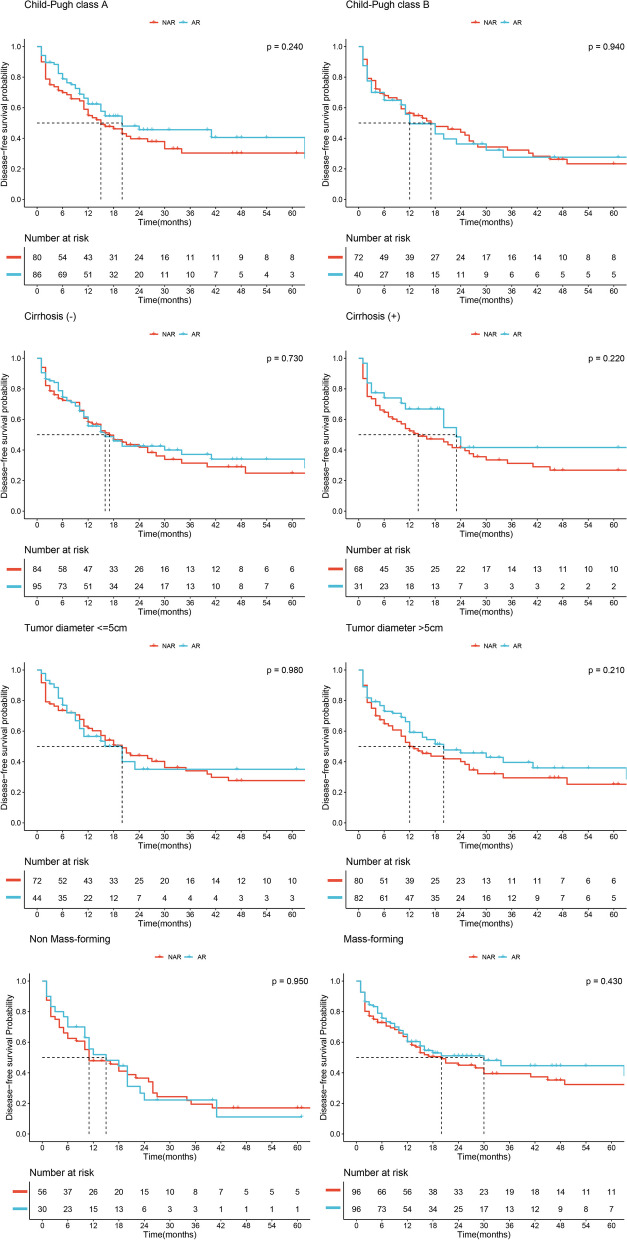
Two hundred seventy-eight ICC patients staged at AJCC I were eligible for this study, including 126 patients receiving AR and 152 patients receiving NAR. Compared to the NAR group, the AR group experienced more intraoperative blood loss before and after PSM or stabilized IPTW (all P > 0.05); AR group also experienced more intraoperative transfusion after stabilized IPTW (P > 0.05). In terms of disease-free survival (DFS) and overall survival (OS), no significant differences were observed between the two groups before and after PSM or stabilized IPTW (all P > 0.05). Multivariable Cox regression analyses found that AR was not an independent prognostic factor for either DFS or OS (all P > 0.05). Further analysis also showed that the survival benefit of AR was not found in any subgroup stratified by Child-Pugh grade (A or B), cirrhosis (presence or absence), tumor diameter (≤ 5 cm or > 5 cm) and pathological type (mass-forming or non-mass-forming) with all P > 0.05.
Surgical approach does not influence the prognosis of patients with stage I primary ICC, and NAR might be acceptable and oncological safety.
根治性切除术仍然是治疗肝内胆管癌(ICC)最具成本效益的策略,但解剖性切除术(AR)的生存获益仍存在争议。本研究旨在比较 AR 与非解剖性切除术(NAR)作为早期 ICC 患者的主要治疗方法的肿瘤学结果。
回顾性收集了 2012 年 12 月至 2015 年 12 月期间中国 12 个肝胆中心接受肝切除术并分期为 AJCC I 期的 ICC 患者数据。采用倾向评分匹配(PSM)和稳定逆概率治疗加权(IPTW)分析来最小化潜在混杂因素的影响,并比较 AR 组和 NAR 组的围手术期和长期结果。
本研究共纳入 278 例 AJCC I 期 ICC 患者,其中 126 例接受 AR,152 例接受 NAR。与 NAR 组相比,PSM 或稳定 IPTW 前后 AR 组术中出血量更多(均 P>0.05);稳定 IPTW 后 AR 组术中输血更多(P>0.05)。在无病生存(DFS)和总生存(OS)方面,PSM 或稳定 IPTW 前后两组之间无显著差异(均 P>0.05)。多变量 Cox 回归分析发现,AR 不是 DFS 或 OS 的独立预后因素(均 P>0.05)。进一步分析还表明,在根据 Child-Pugh 分级(A 或 B)、肝硬化(存在或不存在)、肿瘤直径(≤5cm 或>5cm)和病理类型(肿块型或非肿块型)分层的任何亚组中,AR 的生存获益均未发现(均 P>0.05)。
手术方式并不影响 I 期原发性 ICC 患者的预后,NAR 可能是可接受的且具有肿瘤学安全性。