Division of Rheumatology, Department of Internal Medicine, Keio University School of Medicine, 35 Shinano-machi, Shinjuku-ku, Tokyo, 160-8582, Japan.
Quality and Pharmacovigilance Division, Pharmaceuticals Group, Nippon Kayaku Co., Ltd., 2-1-1 Marunouchi, Chiyoda-ku, Tokyo, 100-0005, Japan.
Drug Saf. 2023 Oct;46(10):991-1005. doi: 10.1007/s40264-023-01340-1. Epub 2023 Sep 12.
Biosimilar CT-P13 was approved with limited data from clinical trials compared to the originator infliximab in biologic-naïve patients with rheumatoid arthritis. Three prospective post-marketing surveillance studies have been conducted in Japanese biologic-naïve patients and switched patients from biologics including the originator infliximab.
We performed an integrated analysis of final data from three post-marketing studies to provide long-term safety and efficacy data of CT-P13 in a real-world clinical setting.
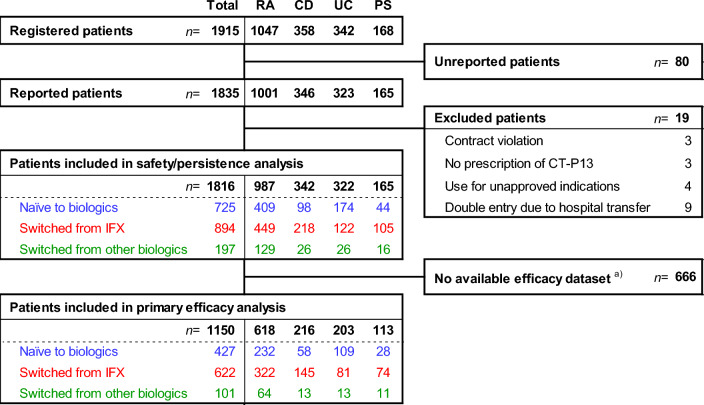
A total of 1816 patients consisting of 987 patients with rheumatoid arthritis, 342 patients with Crohn's disease, 322 patients with ulcerative colitis, and 165 patients with psoriasis were evaluated for safety. Efficacy was assessed in 1150 patients whose disease parameter values were serially collected.
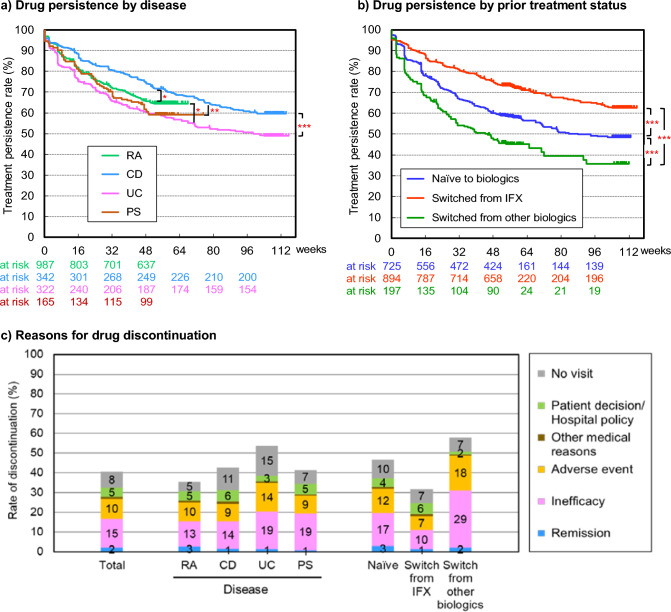
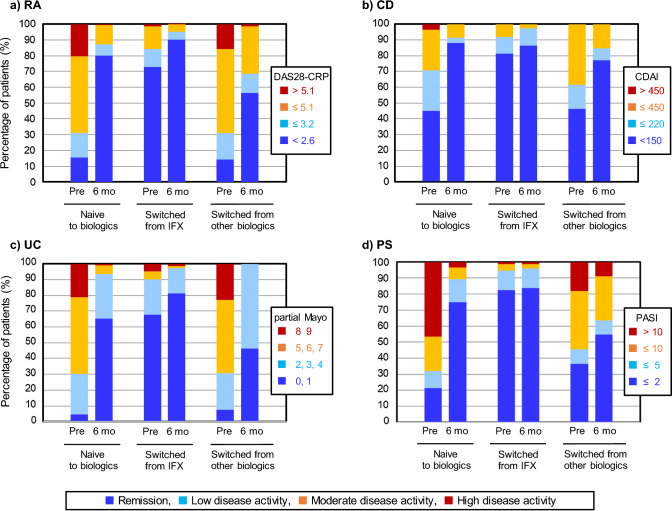
Adverse drug reactions were reported in 24.2% of all patients. The incidence of adverse drug reactions differed by the prior treatment status with biologics: 30.5% in patients naïve to biologics, 17.0% in patients switched from the originator infliximab, and 33.5% in patients switched from other biologics. Infusion reactions were the most frequent adverse drug reactions (8.2%), and its incidence was significantly higher in patients with ulcerative colitis and an allergy history in a multivariable Cox regression analysis. Infection was the second most frequent (6.1%), but tuberculosis only occurred in four patients (0.2%). The incidence of infection was low in patients with Crohn's disease and psoriasis, and significant risk factors were an allergy history, comorbidities, and concomitant steroid use. Interstitial lung disease occurred in 16 patients (0.9%), including 11 patients with rheumatoid arthritis. With CT-P13 therapy, disease activity parameters decreased similarly in all four diseases, although long-term drug discontinuation rates because of inefficacy varied by disease. In naïve patients, the disease activity parameters decreased rapidly and the proportion of patients in remission increased. Patients switched from infliximab maintained lowered parameter levels with infliximab pretreatment. Decreases were also observed in patients switched from other biologics, but discontinuations were most often because of insufficient efficacy.
The integrated analysis of a large number of patients detected no new safety signals with long-term CT-P13 treatment. Efficacy in rheumatoid arthritis, psoriasis, Crohn's disease, and ulcerative colitis cases was confirmed in biologic-naïve patients and switched patients from the originator infliximab or other biologics.
与生物制剂初治患者的原研英夫利昔单抗相比,生物类似药 CT-P13 在类风湿关节炎患者的临床试验中仅提供了有限的数据便获得了批准。三项前瞻性上市后监测研究已经在日本生物制剂初治患者和转换患者中进行,这些患者来自包括原研英夫利昔单抗在内的生物制剂。
我们对三项上市后研究的最终数据进行了综合分析,以提供 CT-P13 在真实临床环境下的长期安全性和疗效数据。
共评估了 1816 名患者的安全性,其中包括 987 名类风湿关节炎患者、342 名克罗恩病患者、322 名溃疡性结肠炎患者和 165 名银屑病患者。1150 名患者的疾病参数值连续收集,用于评估疗效。
所有患者中报告了 24.2%的药物不良反应。药物不良反应的发生率因先前的生物制剂治疗状态而异:生物制剂初治患者为 30.5%、原研英夫利昔单抗转换患者为 17.0%、其他生物制剂转换患者为 33.5%。输注反应是最常见的药物不良反应(8.2%),在溃疡性结肠炎和过敏史患者的多变量 Cox 回归分析中,其发生率显著更高。感染是第二常见的不良反应(6.1%),但在四名患者(0.2%)中发生了结核病。克罗恩病和银屑病患者的感染发生率较低,过敏史、合并症和同时使用皮质类固醇是显著的风险因素。间质性肺病在 16 名患者(0.9%)中发生,其中包括 11 名类风湿关节炎患者。使用 CT-P13 治疗时,四种疾病的疾病活动参数均相似下降,尽管因疗效不佳而长期停药的比例因疾病而异。在初治患者中,疾病活动参数迅速下降,缓解患者的比例增加。从英夫利昔单抗转换的患者在英夫利昔单抗预处理后维持较低的参数水平。从其他生物制剂转换的患者也观察到了下降,但停药主要是因为疗效不足。
对大量患者进行的综合分析未发现长期使用 CT-P13 治疗的新安全性信号。在生物制剂初治患者和从原研英夫利昔单抗或其他生物制剂转换的患者中,确认了类风湿关节炎、银屑病、克罗恩病和溃疡性结肠炎病例的疗效。