Gude Martin, Kirkegaard Hans, Blauenfeldt Rolf, Behrndtz Anne, Mainz Jeppe, Riddervold Ingunn, Simonsen Claus Z, Hjort Niels, Johnsen Søren P, Andersen Grethe, Valentin Jan Brink
Department of Research and Development, Prehospital Emergency Medical Services, Central Denmark Region; and Aarhus University Hospital, Aarhus, Denmark.
Department of Clinical Medicine, Aarhus University, Aarhus, Denmark.
Clin Epidemiol. 2023 Sep 7;15:957-968. doi: 10.2147/CLEP.S418253. eCollection 2023.
To examine the agreement between emergency medical service (EMS) providers, neurology residents and neurology consultants, using the Cincinnati Prehospital Stroke Scale (CPSS) and the Prehospital Acute Stroke Severity Scale (PASS).
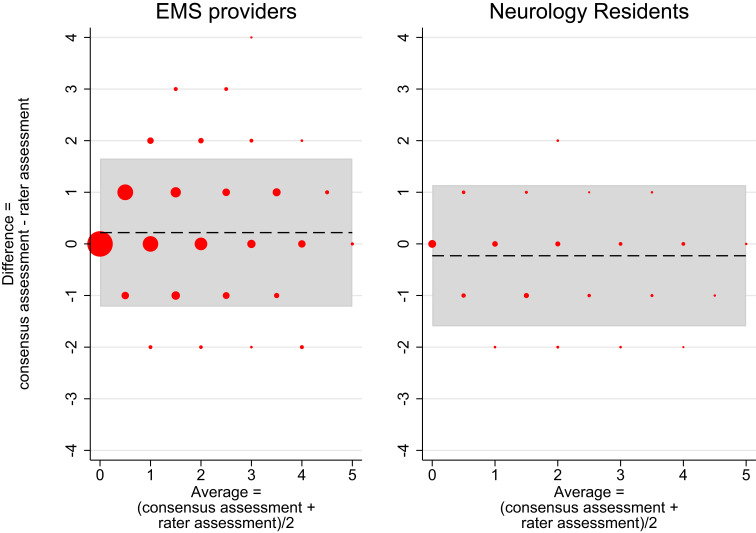
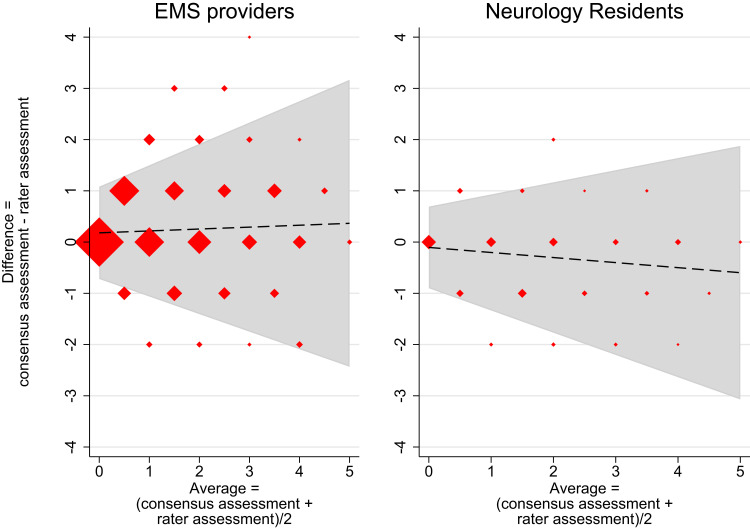
Patients with stroke, transient ischemic attack (TIA) and stroke mimic were included upon primary stroke admission or during rehabilitation. Patients were included from June 2018 to September 2019. Video recordings were made of patients being assessed with CPSS and PASS. The recordings were later presented to the healthcare professionals. To determine relative and absolute interrater reliability in terms of inter-rater agreement (IRA), we used generalisability theory. Group-level agreement was determined against a gold standard and presented as an area under the curve (AUC). The gold standard was a consensus agreement between two neurology consultants.
A total of 120 patient recordings were assessed by 30 EMS providers, two neurology residents and two neurology consultants. Using the CPSS and the PASS, a total of 1,800 assessments were completed by EMS providers, 240 by neurology residents and 240 by neurology consultants. The overall relative and absolute IRA for all items combined from the CPSS and PASS score was 0.84 (95% CI 0.80; 0.87) and 0.81 (95% CI 0.77; 0.85), respectively. Using the CPSS, the agreement on a group-level resulted in AUCs of 0.83 (95% CI 0.78; 0.88) for the EMS providers and 0.86 (95% CI 0.82; 0.90) for the neurology residents when compared with the gold standard. Using the PASS, the AUC was 0.82 (95% CI 0.77; 0.87) for the EMS providers and 0.88 (95% CI 0.84; 0.93) for the neurology residents.
The high relative and absolute inter-rater agreement underpins a high robustness/generalisability of the two scales. A high agreement exists across individual raters and different groups of healthcare professionals supporting widespread applicability of the stroke scales.
使用辛辛那提院前卒中量表(CPSS)和院前急性卒中严重程度量表(PASS),检验急救医疗服务(EMS)提供者、神经内科住院医师和神经内科顾问之间的一致性。
纳入初次卒中入院或康复期间的卒中、短暂性脑缺血发作(TIA)和疑似卒中患者。纳入2018年6月至2019年9月期间的患者。对使用CPSS和PASS评估患者的过程进行录像。录像随后展示给医疗专业人员。为了根据评分者间一致性(IRA)确定相对和绝对评分者信度,我们使用了概化理论。根据金标准确定组间一致性,并以曲线下面积(AUC)表示。金标准是两位神经内科顾问之间的共识性意见。
30名EMS提供者、两名神经内科住院医师和两名神经内科顾问共评估了120份患者录像。使用CPSS和PASS,EMS提供者共完成了1800次评估,神经内科住院医师完成了240次评估,神经内科顾问完成了240次评估。CPSS和PASS评分所有项目综合的总体相对和绝对IRA分别为0.84(95%CI 0.80;0.87)和0.81(95%CI 0.77;0.85)。使用CPSS时,与金标准相比,EMS提供者组间一致性的AUC为0.83(95%CI 0.78;0.88),神经内科住院医师为0.86(95%CI 0.82;0.90)。使用PASS时(与金标准相比),EMS提供者的AUC为0.82(95%CI 0.77;0.87),神经内科住院医师为0.88(95%CI 0.84;0.93)。
较高的相对和绝对评分者间一致性支持了这两个量表的高稳健性/可推广性。个体评分者和不同医疗专业人员群体之间存在高度一致性,支持卒中量表的广泛适用性。