Carolina Urologic Research Center, 823 82nd Pkwy, Suite B, Myrtle Beach, SC, 29572, USA.
Oregon Urology Institute, Springfield, OR, USA.
Adv Ther. 2023 Nov;40(11):4919-4927. doi: 10.1007/s12325-023-02634-7. Epub 2023 Sep 15.
Cardiovascular (CV) events are the leading cause of death in prostate cancer. Men with prostate cancer are likely to have CV risk factors and use CV-related concomitant medications. In the phase 3 HERO study, a 54% lower incidence of major adverse cardiac events was reported in men treated with the oral gonadotropin-releasing hormone (GnRH) receptor antagonist, relugolix, vs leuprolide. Herein, we characterize the impact of concomitant CV therapies on efficacy and safety in the HERO study.
In HERO, 930 men with advanced prostate cancer (APC) were randomized 2:1 and treated with relugolix (120 mg orally once daily; after single 360 mg loading dose) or leuprolide (injections every 3 months) for 48 weeks. Subgroups analyzed included men who received antihypertensives, antithrombotics, or lipid-modifying therapies (LMAs), as well as the most common drug classes (> 10%) and single most common agent within each class. Assessments included sustained testosterone suppression to castrate levels (< 50 ng/dL) through 48 weeks and safety.
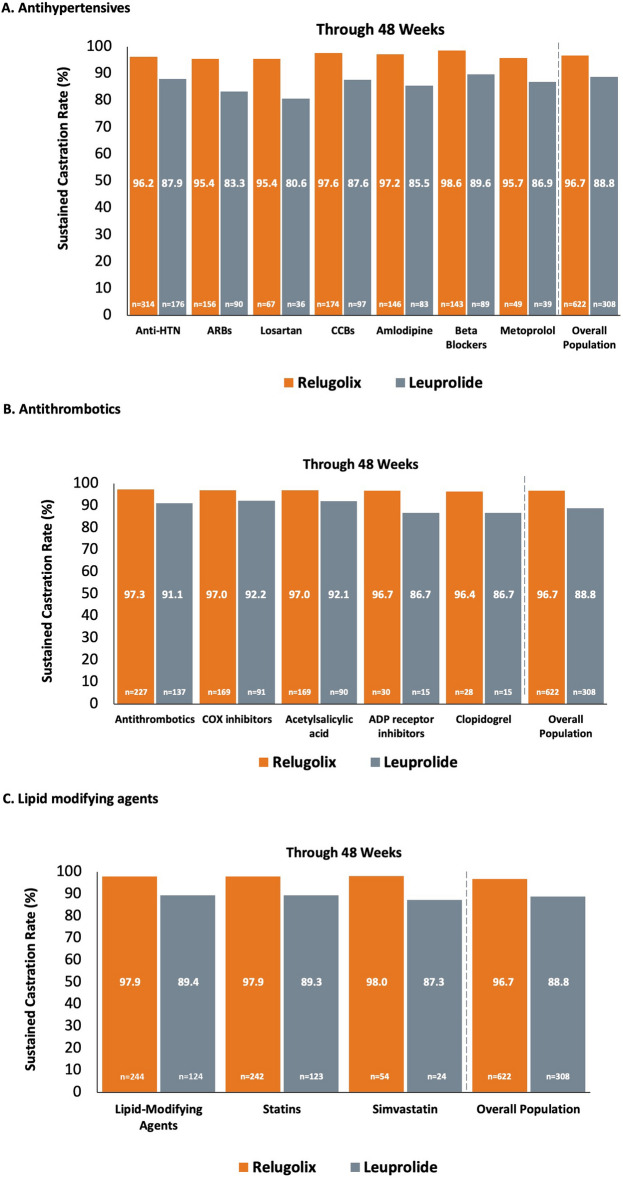
Antihypertensives, antithrombotics, and LMAs were utilized by 52.7%, 39.1%, and 39.6% of men in HERO, respectively. In the main subgroups, point estimates for sustained castration rates were generally consistent with overall estimates of relugolix and leuprolide observed in the overall population. Sustained castration rates were also mostly consistent for men taking the most common drug classes and individual agents in each class (losartan [n = 103]: relugolix, 95.4% vs leuprolide, 80.6%; amlodipine [n = 229]: 97.2% vs 85.5%; metoprolol [n = 88]: 95.7% vs 86.9%; acetylsalicylic acid [n = 259]: 97.0% vs 92.1%; clopidogrel [n = 43]: 96.4% vs 86.7%; simvastatin [n = 78]: 98.0% vs 87.3%). Incidence and types of adverse events (AEs) among men who received these medications were mostly consistent with overall population results, with some increases in grade ≥ 3 and fatal AEs.
Relugolix suppressed testosterone and was generally well tolerated when given with concomitant CV agents.
Clinical Trial ID NCT03085095.
Data presented at 15th Annual Genitourinary Cancers Symposium; February 17-19, 2022, San Francisco, CA, USA [Abstract 101, Poster board E11]. The published abstract from this presentation can be found at https://ascopubs.org/doi/10.1200/JCO.2022.40.6_suppl.101 .
心血管(CV)事件是前列腺癌患者死亡的主要原因。患有前列腺癌的男性可能存在 CV 危险因素,并使用与 CV 相关的伴随药物。在 3 期 HERO 研究中,与使用亮丙瑞林相比,口服促性腺激素释放激素(GnRH)受体拮抗剂瑞戈非尼治疗的男性发生主要不良心脏事件的发生率降低了 54%。在此,我们描述了伴随 CV 治疗对 HERO 研究中疗效和安全性的影响。
在 HERO 中,930 名晚期前列腺癌(APC)男性患者被随机分为 2:1 组,分别接受瑞戈非尼(120mg 口服,每日一次;单次 360mg 负荷剂量后)或亮丙瑞林(每 3 个月注射一次)治疗 48 周。分析的亚组包括接受抗高血压药物、抗血栓药物或调脂治疗(LMAs)的男性,以及最常见的药物类别(>10%)和每个类别中最常见的单一药物。评估包括通过 48 周持续达到去势水平(<50ng/dL)的睾酮抑制情况和安全性。
抗高血压药物、抗血栓药物和 LMAs 在 HERO 中分别被 52.7%、39.1%和 39.6%的男性使用。在主要亚组中,持续去势率的点估计值与总体人群中观察到的瑞戈非尼和亮丙瑞林的总体估计值基本一致。服用最常见药物类别和每个类别中最常见药物的男性的持续去势率也基本一致(氯沙坦[n=103]:瑞戈非尼 95.4% vs 亮丙瑞林 80.6%;氨氯地平[n=229]:97.2% vs 85.5%;美托洛尔[n=88]:95.7% vs 86.9%;乙酰水杨酸[n=259]:97.0% vs 92.1%;氯吡格雷[n=43]:96.4% vs 86.7%;辛伐他汀[n=78]:98.0% vs 87.3%)。接受这些药物治疗的男性发生不良事件(AE)的发生率和类型与总体人群结果基本一致,某些严重程度≥3 级和致命 AE 的发生率有所增加。
瑞戈非尼抑制睾酮,与伴随的 CV 药物联合使用时通常具有良好的耐受性。
临床试验 ID NCT03085095。
在第 15 届泌尿生殖系统癌症研讨会;2022 年 2 月 17-19 日,美国旧金山,CA,美国[摘要 101,海报板 E11]。本次会议的已发表摘要可在以下网址找到:https://ascopubs.org/doi/10.1200/JCO.2022.40.6_suppl.101。