García-Padilla Paola, Dávila-Rúales Valentina, Hurtado Diana C, Vargas Diana C, Muñoz Oscar M, Jurado Mayra A
Department of Internal Medicine, Pontificia Universidad Javeriana, Hospital Universitario San Ignacio, Bogotá, Colombia.
Unit of Nephrology, Pontificia Universidad Javeriana, Hospital Universitario San Ignacio, Bogotá, Colombia.
Can J Kidney Health Dis. 2023 Sep 14;10:20543581231199011. doi: 10.1177/20543581231199011. eCollection 2023.
Patients with diabetes mellitus (DM) have worse graft and overall survival, but recent evidence suggests that the difference is no longer significant.
To compare the outcomes between patients with end-stage kidney disease due to DM (ESKD-DM) and ESKD due to nondiabetic etiology (ESKD-non-DM) who underwent kidney transplantation (KT) up to 10 years of follow-up.
Survival analysis of a retrospective cohort.
All patients who underwent KT at the Hospital Universitario San Ignacio, Colombia, between 2004 and 2022.
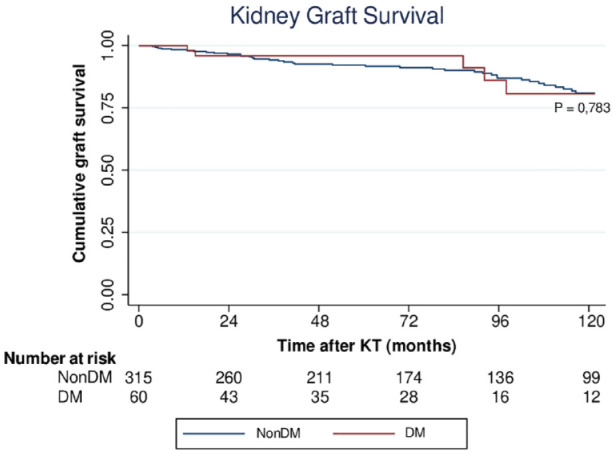
Overall and graft survival in ESKD-DM and ESKD-non-DM who received KT. Patients who died with functional graft were censored for the calculation of kidney graft survival.
Log-rank test, Cox proportional hazards model, and competing risk analysis were used to compare overall and graft survival in patients with ESKD-DM and ESKD-non-DM who underwent KT.
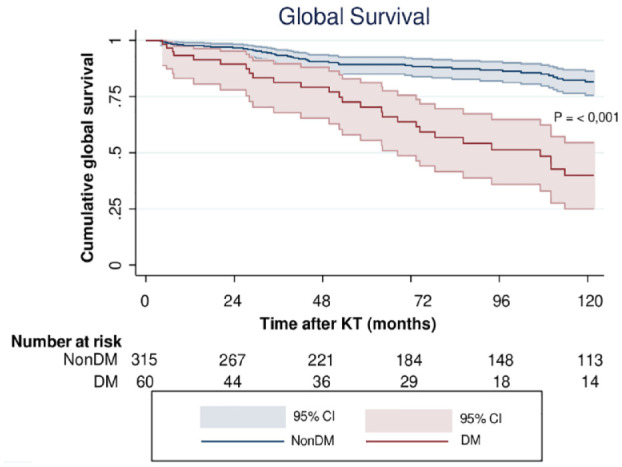
A total of 375 patients were included: 60 (16%) with ESKD-DM and 315 (84%) with ESKD-non-DM. Median follow-up was 83.3 months. Overall survival was lower in patients with ESKD-DM at 5 (75.0% vs 90.8%, < .001) and 10 years (55.0% vs 86.7%, < .001). Cardiovascular death was higher in patients with diabetes (27.3% vs 8.2%, = .021). Death-censored graft survival was similar in both groups (96.7% vs 93.3% at 5 years, = .324). On multivariate analysis, the factors associated with global survival were DM (hazard ratio [HR] = 2.11, 95% confidence interval [CI] = 1.23-3.60, = .006), recipient age (HR = 1.05, 95% CI = 1.02-1.08, < .001), delayed graft function (HR = 2.07, 95% CI = 1.24-3.46, = .005), and donor age (HR = 1.03, 95% CI = 1.01-1.05, = .002). In the competing risk analysis, DM was associated with mortality only in the cardiovascular death group (sub-hazard ratio [SHR] = 6.06, 95% CI = 1.01-36.4, = .049).
Change in diabetes treatment received over time and adherence to glycemic targets were not considered. The sample size is relatively small, which limits the precision of our estimates. The Kidney Donor Profile Index and the occurrence of treated acute rejection were not included in the regression models.
Overall survival is lower in patients with diabetes, possibly due to older age and cardiovascular comorbidities. Therefore, patients with diabetes should be followed more closely to control cardiovascular risk factors. However, there is no difference in graft survival.
糖尿病(DM)患者的移植物和总体生存率较差,但最近的证据表明这种差异已不再显著。
比较糖尿病所致终末期肾病(ESKD-DM)患者和非糖尿病病因所致终末期肾病(ESKD-非DM)患者在接受肾移植(KT)后长达10年随访期间的预后情况。
回顾性队列的生存分析。
2004年至2022年期间在哥伦比亚圣伊格纳西奥大学医院接受KT的所有患者。
接受KT的ESKD-DM和ESKD-非DM患者的总体生存率和移植物生存率。计算肾移植物生存率时,对有功能移植物的死亡患者进行截尾。
采用对数秩检验、Cox比例风险模型和竞争风险分析,比较接受KT的ESKD-DM和ESKD-非DM患者的总体生存率和移植物生存率。
共纳入375例患者:60例(16%)为ESKD-DM患者,315例(84%)为ESKD-非DM患者。中位随访时间为83.3个月。ESKD-DM患者在5年(75.0%对90.8%,P<.001)和10年(55.0%对86.7%,P<.001)时的总体生存率较低。糖尿病患者的心血管死亡发生率较高(27.3%对8.2%,P=.021)。两组的死亡截尾移植物生存率相似(5年时为96.7%对93.3%,P=.324)。多因素分析显示,与总体生存相关的因素包括糖尿病(风险比[HR]=2.11,95%置信区间[CI]=1.23-3.60,P=.006)、受者年龄(HR=1.05,95%CI=1.02-1.08,P<.001)、移植肾功能延迟(HR=2.07,95%CI=1.24-3.46,P=.005)和供者年龄(HR=1.03,95%CI=1.01-1.05,P=.002)。在竞争风险分析中,糖尿病仅与心血管死亡组的死亡率相关(亚风险比[SHR]=6.06,95%CI=1.01-36.4,P=.049)。
未考虑随时间推移接受的糖尿病治疗变化以及对血糖目标的依从性。样本量相对较小,这限制了我们估计的精度。回归模型未纳入肾脏供者特征指数和治疗性急性排斥反应的发生情况。
糖尿病患者的总体生存率较低,可能是由于年龄较大和心血管合并症。因此,应更密切地随访糖尿病患者以控制心血管危险因素。然而,移植物生存率没有差异。