Rodgers-Melnick Samuel N, Rivard Rachael L, Block Seneca, Dusek Jeffery A
Connor Whole Health, University Hospitals of Cleveland, Cleveland, OH, USA.
School of Medicine, Case Western Reserve University, Cleveland, OH, USA.
Pain Rep. 2023 Apr 13;8(3):e1074. doi: 10.1097/PR9.0000000000001074. eCollection 2023 May-Jun.
Given the challenges health systems face in providing effective nonpharmacologic treatment for pain and psychological distress, clinical effectiveness studies of evidence-based strategies such as music therapy (MT) are needed.
This study examined changes in patient-reported outcomes (PROs) after MT and explored variables associated with pain reduction of ≥2 units on a 0 to 10 numeric rating scale (NRS).
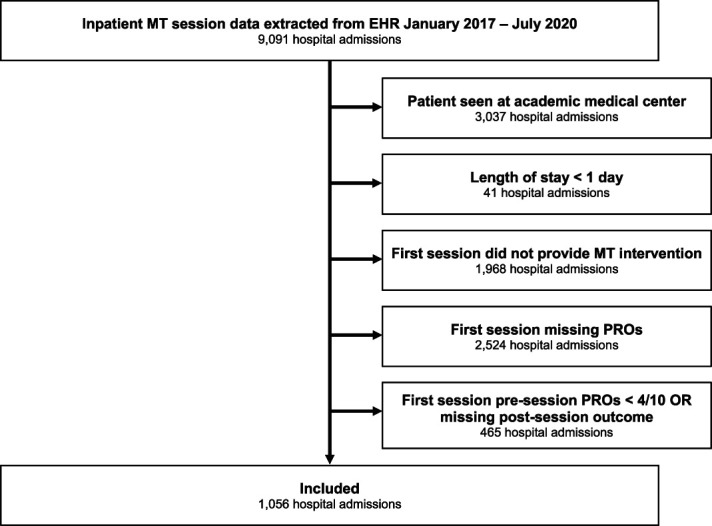
A retrospective review was conducted on initial MT interventions provided to adults receiving community hospital care between January 2017 and July 2020. Sessions were included if participants reported pre-session pain, anxiety, and/or stress scores of ≥4 on the NRS. Data analysis included a bootstrap analysis of single-session changes in PROs and a logistic regression exploring variables associated with pain reduction (ie, ≥2 units vs <2 units).
Patients (n = 1056; mean age: 63.83 years; 76.1% female; 57.1% White; 41.1% Black/African American) reported clinically significant mean reductions in pain (2.04 units), anxiety (2.80 units), and stress (3.48 units). After adjusting for demographic, clinical, and operational characteristics in the model (c-statistic = 0.668), patients receiving an MT session in which pain management was a goal were 4.32 times more likely (95% confidence interval 2.26, 8.66) to report pain reduction of ≥2 units than patients receiving an MT session in which pain management was not a session goal.
This retrospective study supports the clinical effectiveness of MT for symptom management in community hospitals. However, additional research is needed to determine which characteristics of MT interventions and patients influence pain change.
鉴于卫生系统在提供有效的疼痛和心理困扰非药物治疗方面面临挑战,因此需要对音乐疗法(MT)等循证策略进行临床有效性研究。
本研究调查了MT后患者报告结局(PROs)的变化,并探索了与数字评分量表(NRS)上疼痛减轻≥2分相关的变量。
对2017年1月至2020年7月期间接受社区医院护理的成年人所接受的初始MT干预进行回顾性分析。如果参与者报告NRS上的会前疼痛、焦虑和/或压力评分≥4分,则纳入这些疗程。数据分析包括对PROs单疗程变化的自抽样分析,以及探索与疼痛减轻(即≥2分与<2分)相关变量的逻辑回归分析。
患者(n = 1056;平均年龄:63.83岁;76.1%为女性;57.1%为白人;41.1%为黑人/非裔美国人)报告疼痛(2.04分)、焦虑(2.80分)和压力(3.48分)的临床显著平均减轻。在对模型中的人口统计学、临床和操作特征进行调整后(c统计量 = 0.668),以疼痛管理为目标接受MT疗程的患者报告疼痛减轻≥2分的可能性是未将疼痛管理作为疗程目标的患者的4.32倍(95%置信区间2.26,8.66)。
这项回顾性研究支持MT在社区医院症状管理中的临床有效性。然而,需要进一步研究以确定MT干预措施和患者的哪些特征会影响疼痛变化。