Department of Internal Medicine, Beth Israel Deaconess Medical Center, Boston, MA.
Harvard Medical School, Boston, MA.
Blood Adv. 2023 Dec 26;7(24):7516-7524. doi: 10.1182/bloodadvances.2023011235.
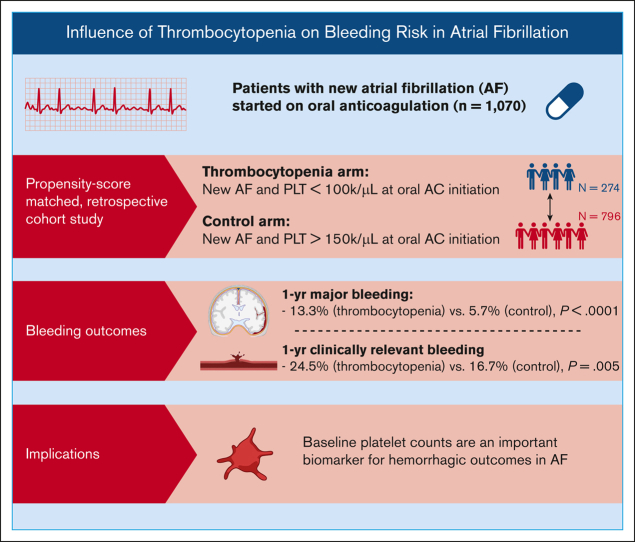
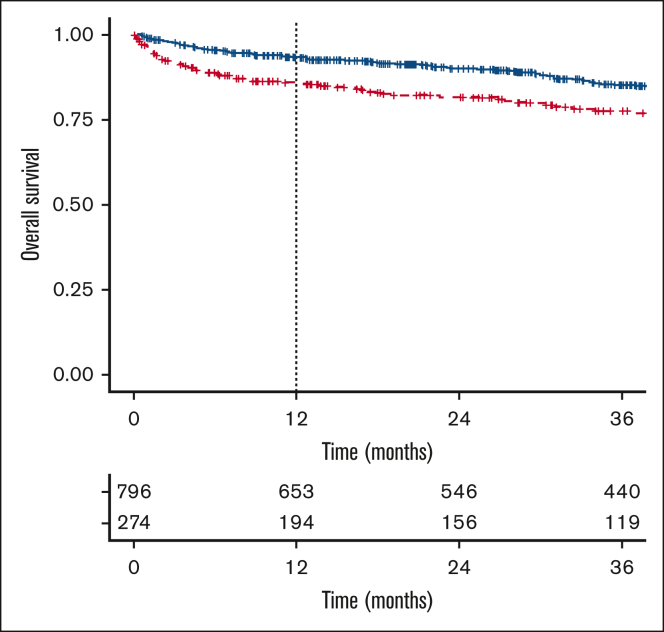
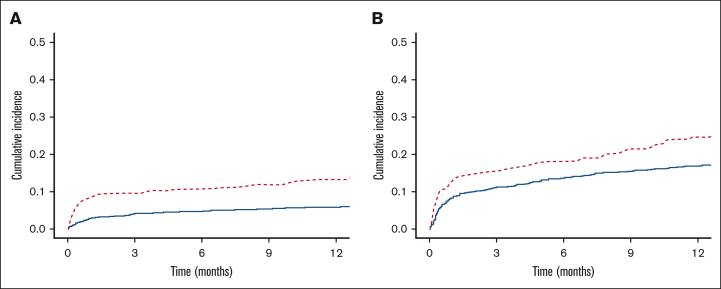
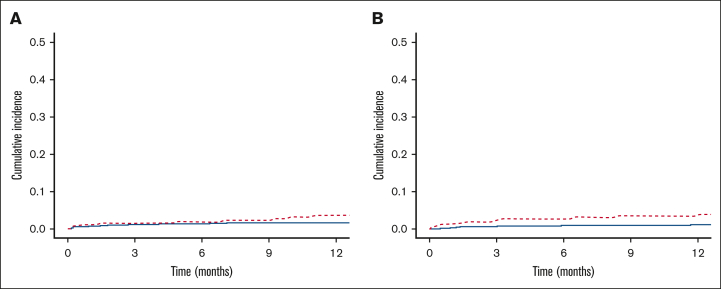
Whether thrombocytopenia substantively increases the risk of hemorrhage associated with anticoagulation in patients with atrial fibrillation (AF) is not established. The purpose of this study was to compare rates of bleeding in patients with AF and thrombocytopenia (platelet count < 100 000/μL) to patients with AF and normal platelet counts (>150 000/μL). We performed a propensity score-matched, retrospective cohort study of adults (n = 1070) with a new diagnosis of AF who received a prescription for an oral anticoagulant between 2015 and 2020. The thrombocytopenia cohort was defined as having at least 2 platelet counts <100 000/μL on separate days in the period spanning the 12 weeks preceding the initiation of anticoagulation to 6 weeks after the initiation of anticoagulation. The primary end point was the 1-year cumulative incidence of major bleeding; secondary end points included clinically relevant bleeding, arterial and venous thrombotic events, and all-cause mortality. Patients with AF and thrombocytopenia experienced a higher 1-year cumulative incidence of major bleeding (13.3% vs 5.7%; P < .0001) and clinically relevant bleeding (24.5% vs 16.7%; P = .005) than the controls. Thrombocytopenia was identified as an independent risk factor for major bleeding (hazard ratio, 2.20; confidence interval, 1.36-3.58; P = .001), with increasing risk based on the severity of thrombocytopenia. The cumulative incidence of arterial thrombosis at 1 year was 3.6% in the group with thrombocytopenia and 1.5% in controls (Gray test, P = .08). These findings suggest that baseline platelet counts are an important biomarker for hemorrhagic outcomes in AF and that the degree of thrombocytopenia is an important factor in determining the level of risk.
血小板减少是否实质性增加了伴有心房颤动(AF)的抗凝治疗相关出血的风险尚不确定。本研究的目的是比较伴有血小板减少症(血小板计数<100,000/μL)和正常血小板计数(>150,000/μL)的 AF 患者的出血率。我们对 2015 年至 2020 年期间接受口服抗凝剂治疗的新诊断为 AF 的成年人(n=1070)进行了倾向评分匹配的回顾性队列研究。血小板减少症组的定义为在抗凝治疗开始前 12 周至抗凝治疗开始后 6 周的时间内,至少有 2 次血小板计数<100,000/μL。主要终点是 1 年累积大出血发生率;次要终点包括临床相关出血、动脉和静脉血栓栓塞事件以及全因死亡率。伴有 AF 和血小板减少症的患者 1 年累积大出血发生率(13.3% vs. 5.7%;P<0.0001)和临床相关出血发生率(24.5% vs. 16.7%;P=0.005)均高于对照组。血小板减少症是大出血的独立危险因素(风险比,2.20;置信区间,1.36-3.58;P=0.001),且随着血小板减少症的严重程度增加,风险也随之增加。伴有血小板减少症的患者 1 年时动脉血栓形成的累积发生率为 3.6%,对照组为 1.5%(Gray 检验,P=0.08)。这些发现表明,基线血小板计数是 AF 出血结局的重要生物标志物,血小板减少症的程度是确定风险水平的重要因素。