School of Population Health, Institute of Global Surgery, RCSI University of Medicine and Health Sciences, Dublin, Ireland.
Nuffield Department of Orthopedics, Rheumatology and Musculoskeletal Sciences, University of Oxford, Oxford, United Kingdom.
Front Public Health. 2023 Sep 14;11:1186307. doi: 10.3389/fpubh.2023.1186307. eCollection 2023.
In 2017 the SURG-Africa project set out to institute a surgical, obstetric, trauma and anesthesia (SOTA) care capacity-building intervention focused on non-specialist providers at district hospitals in Zambia, Malawi and Tanzania. The aim was to scale up quality-assured SOTA care for rural populations. This paper reports the process of developing the intervention and our experience of initial implementation, using a participatory approach.
Participatory Action Research workshops were held in the 3 countries in July-October 2017 and in October 2018-July 2019, involving representatives of key local stakeholder groups: district hospital (DH) surgical teams and administrators, referral hospital SOTA specialists, professional associations and local authorities. Through semi-structured discussions, qualitative data were collected on participants' perceptions and experiences of barriers to the provision of SOTA care at district level, and on the training and supervision needs of district surgical teams. Data were compared for themes across countries and across surgical team cadres.
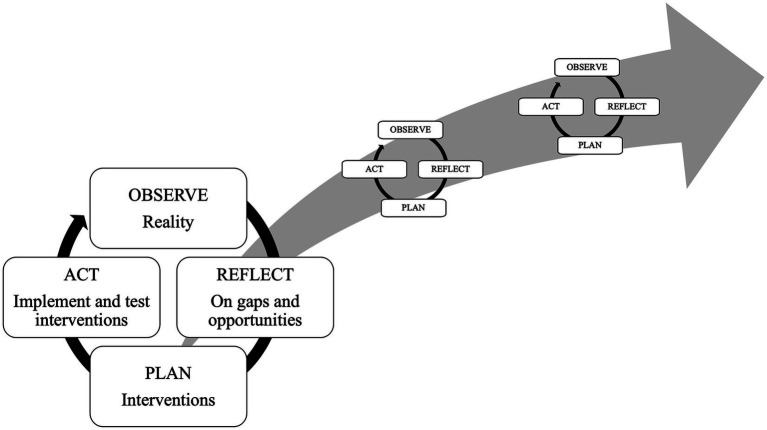
All groups reported a lack of in-service training to develop essential skills to manage common SOTA cases; use and care of equipment; essential anesthesia care including resuscitation skills; and infection prevention and control. Very few district surgical teams had access to supervision. SOTA providers at DHs reported a demand for more feedback on referrals. Participants prioritized training needs that could be addressed through regular in-service training and supervision visits from referral hospital specialists to DHs. These data were used by participants in an action-planning cycle to develop site-specific training plans for each research site.
The inclusive, participatory approach to stakeholder involvement in SOTA system strengthening employed by this study supported the design of a locally relevant and contextualized intervention. This study provides lessons on how to rebalance power dynamics in Global Surgery, through giving a voice to district surgical teams.
2017 年,SURG-Africa 项目着手实施一项外科、产科、创伤和麻醉(SOTA)护理能力建设干预措施,重点是赞比亚、马拉维和坦桑尼亚的地区医院的非专业提供者。目的是为农村人口扩大质量保证的 SOTA 护理。本文报告了干预措施的制定过程,以及我们在使用参与式方法实施初期的经验。
2017 年 7 月至 10 月和 2018 年 10 月至 2019 年 7 月,在 3 个国家举行了参与式行动研究研讨会,参与者包括当地主要利益攸关方群体的代表:地区医院(DH)外科团队和管理人员、转诊医院 SOTA 专家、专业协会和地方当局。通过半结构化讨论,收集了关于参与者对地区一级提供 SOTA 护理的障碍的看法和经验,以及对地区外科团队的培训和监督需求的定性数据。对各国和外科团队干部的主题进行了比较。
所有团体都报告说,缺乏在职培训来发展管理常见 SOTA 病例的基本技能;设备的使用和保养;基本的麻醉护理,包括复苏技能;以及感染预防和控制。很少有地区外科团队能够获得监督。DH 的 SOTA 提供者报告说,需要更多关于转诊的反馈。参与者优先考虑可以通过定期在职培训和转诊医院专家对 DH 进行监督访问来解决的培训需求。这些数据被参与者用于一个行动计划周期,为每个研究地点制定了具体的培训计划。
本研究采用包容性、参与性的方法让利益攸关方参与 SOTA 系统的强化,支持了设计一个具有地方相关性和针对性的干预措施。本研究提供了关于如何通过赋予地区外科团队权力来重新平衡全球外科手术中的权力动态的经验教训。