Department of Hematology, Treant Hospital, Emmen, The Netherlands; Department of Hematology, University Medical Center Groningen, Groningen.
Department of Research and Development, Netherlands Comprehensive Cancer Organisation (IKNL), Utrecht.
Haematologica. 2024 Apr 1;109(4):1163-1170. doi: 10.3324/haematol.2023.283174.
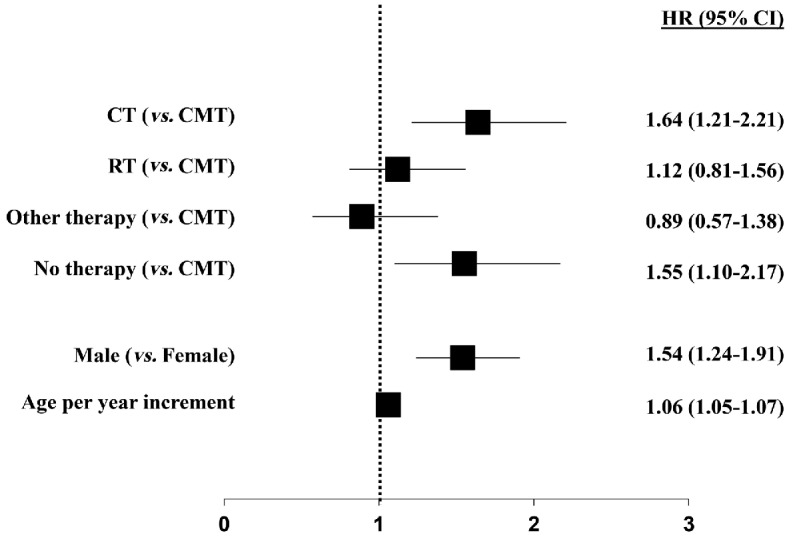
Peripheral T-cell lymphomas (PTCL) comprise a heterogeneous group of mature T-cell neoplasms with an unfavorable prognosis; presentation with stage I(E) disease is uncommon. In clinical practice, an abbreviated chemotherapy treatment regimen combined with radiotherapy (combined modality treatment [CMT]) is commonly used, although evidence from clinical trials is lacking. The aim of this nationwide population-based cohort study is to describe first-line treatment and outcome of patients with stage I(E) PTCL. All newly diagnosed patients ≥18 years with stage I(E) anaplastic large cell lymphoma (ALCL), angioimmunoblastic T-cell lymphoma (AITL) and peripheral T-cell lymphoma NOS (PTCL not otherise specified [NOS]) in 1989-2020 were identified in the Netherlands Cancer Registry. Patients were categorized according to treatment regimen, i.e., chemotherapy (CT), radiotherapy (RT), CMT, other therapy and no treatment. The primary endpoint was overall survival (OS). Patients with stage I(E) ALCL, AITL and PTCL NOS (n=576) were most commonly treated with CMT (28%) or CT (29%), 2% underwent SCT. RT only was given in 18%, and 8% received other therapy and 16% no treatment. Overall, the 5-year OS was 59%. According to subtype, 5-year OS was superior for ALCL as compared to PTCL NOS and AITL (68% vs. 55% and 52%, respectively; P=0.03). For patients treated with CMT, 5-year OS was significantly higher (72%) as compared to patients treated with either CT or RT alone (55% and 55%, respectively; P<0.01). In multivariable analysis, age per year increment (hazard ratio [HR] =1.06, 95% confidence interval [CI]: 1.05-1.07), male sex (HR=1.53, 95% CI: 1.23-1.90), and CT, or no treatment (HR=1.64, 95% CI: 1.21-2.21, and HR=1.55, 95% CI: 1.10-2.17, respectively) were associated with a higher risk of mortality. For stage I(E) ALCL, AITL and PTCL NOS, 5-year OS is 59%, comparing favorably to historical outcome in advanced-stage disease. Superior outcome estimates were observed in patients treated with CMT.
外周 T 细胞淋巴瘤(PTCL)是一组异质性成熟 T 细胞肿瘤,预后不良;I(E)期疾病的表现并不常见。在临床实践中,常采用联合化疗和放疗的简化化疗方案(联合治疗[CMT]),但缺乏临床试验证据。本项全国性基于人群的队列研究旨在描述 I(E)期 PTCL 的一线治疗和结局。在 1989 年至 2020 年间,荷兰癌症登记处确定了所有年龄≥18 岁、诊断为 I(E)期间变性大细胞淋巴瘤(ALCL)、血管免疫母细胞性 T 细胞淋巴瘤(AITL)和外周 T 细胞淋巴瘤非特指型(PTCL 非特指型[NOS])的新诊断患者。根据治疗方案(CT、RT、CMT、其他治疗和未治疗)对患者进行分类。主要终点为总生存期(OS)。I(E)期 ALCL、AITL 和 PTCL NOS 患者(n=576)最常接受 CMT(28%)或 CT(29%)治疗,2%接受 SCT。仅接受 RT 的患者占 18%,8%接受其他治疗,16%未治疗。总体而言,5 年 OS 为 59%。根据亚型,ALCL 的 5 年 OS 优于 PTCL NOS 和 AITL(分别为 68%、55%和 52%;P=0.03)。CMT 治疗患者的 5 年 OS 明显高于 CT 或 RT 单独治疗患者(分别为 72%、55%和 55%;P<0.01)。多变量分析显示,年龄每增加 1 岁(风险比[HR] =1.06,95%置信区间[CI]:1.05-1.07)、男性(HR=1.53,95% CI:1.23-1.90)、CT 或未治疗(HR=1.64,95% CI:1.21-2.21 和 HR=1.55,95% CI:1.10-2.17)与死亡风险增加相关。对于 I(E)期 ALCL、AITL 和 PTCL NOS,5 年 OS 为 59%,与晚期疾病的历史结果相比,这一结果相当乐观。接受 CMT 治疗的患者预后估计更优。