Department of Medicine, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, South Africa.
Khayelitsha District Hospital, Cape Town, South Africa.
PLoS One. 2023 Oct 5;18(10):e0277995. doi: 10.1371/journal.pone.0277995. eCollection 2023.
COVID-19 experiences on noncommunicable diseases (NCDs) from district-level hospital settings during waves I and II are scarcely documented. The aim of this study is to investigate the NCDs associated with COVID-19 severity and mortality in a district-level hospital with a high HIV/TB burden.
This was a retrospective observational study that compared COVID-19 waves I and II at Khayelitsha District Hospital in Cape Town, South Africa. COVID-19 adult patients with a confirmed SARS-CoV-2 polymerase chain reaction (PCR) or positive antigen test were included. In order to compare the inter wave period, clinical and laboratory parameters on hospital admission of noncommunicable diseases, the Student t-test or Mann-Whitney U for continuous data and the X2 test or Fishers' Exact test for categorical data were used. The role of the NCD subpopulation on COVID-19 mortality was determined using latent class analysis (LCA).
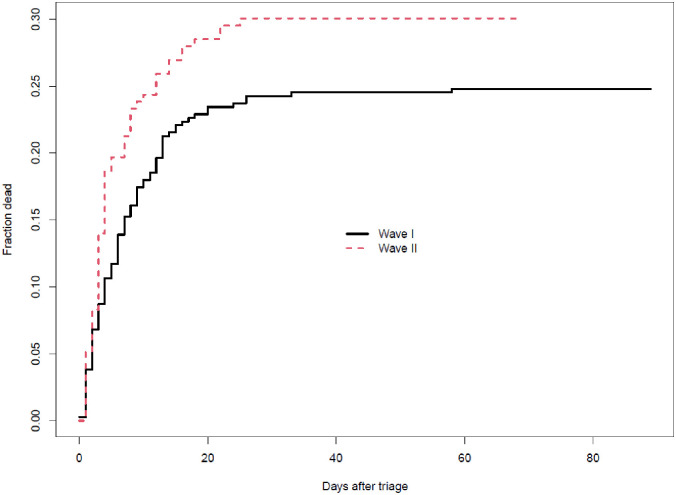
Among 560 patients admitted with COVID-19, patients admitted during wave II were significantly older than those admitted during wave I. The most prevalent comorbidity patterns were hypertension (87%), diabetes mellitus (65%), HIV/AIDS (30%), obesity (19%), Chronic Kidney Disease (CKD) (13%), Congestive Cardiac Failure (CCF) (8.8%), Chronic Obstructive Pulmonary Disease (COPD) (3%), cerebrovascular accidents (CVA)/stroke (3%), with similar prevalence in both waves except HIV status [(23% vs 34% waves II and I, respectively), p = 0.022], obesity [(52% vs 2.5%, waves II and I, respectively), p <0.001], previous stroke [(1% vs 4.1%, waves II and I, respectively), p = 0.046]. In terms of clinical and laboratory findings, our study found that wave I patients had higher haemoglobin and HIV viral loads. Wave II, on the other hand, had statistically significant higher chest radiography abnormalities, fraction of inspired oxygen (FiO2), and uraemia. The adjusted odds ratio for death vs discharge between waves I and II was similar (0.94, 95%CI: 0.84-1.05). Wave I had a longer average survival time (8.0 vs 6.1 days) and a shorter average length of stay among patients discharged alive (9.2 vs 10.7 days). LCA revealed that the cardiovascular phenotype had the highest mortality, followed by diabetes and CKD phenotypes. Only Diabetes and hypertension phenotypes had the lowest mortality.
Even though clinical and laboratory characteristics differed significantly between the two waves, mortality remained constant. According to LCA, the cardiovascular, diabetes, and CKD phenotypes had the highest death probability.
关于 COVID-19 在第一波和第二波期间对非传染性疾病(NCDs)的影响,来自区级医院的数据很少。本研究的目的是调查在一个 HIV/TB 负担沉重的区级医院中,与 COVID-19 严重程度和死亡率相关的 NCDs。
这是一项回顾性观察性研究,比较了南非开普敦 Khayelitsha 地区医院的 COVID-19 第一波和第二波。研究纳入了 COVID-19 成年患者,这些患者的 SARS-CoV-2 聚合酶链反应(PCR)或抗原检测阳性。为了比较两次波之间的差异,使用学生 t 检验或曼-惠特尼 U 检验比较入院时非传染性疾病的临床和实验室参数,使用卡方检验或 Fisher 精确检验比较分类数据。使用潜在类别分析(LCA)确定 NCD 亚群对 COVID-19 死亡率的作用。
在 560 名因 COVID-19 住院的患者中,第二波期间入院的患者明显比第一波期间入院的患者年龄更大。最常见的合并症模式是高血压(87%)、糖尿病(65%)、HIV/AIDS(30%)、肥胖(19%)、慢性肾脏病(CKD)(13%)、充血性心力衰竭(CCF)(8.8%)、慢性阻塞性肺疾病(COPD)(3%)、脑血管意外(CVA)/中风(3%),两种波之间的患病率相似,除了 HIV 状态[(23%比第二波和第一波分别为 34%),p=0.022]、肥胖[(52%比第二波和第一波分别为 2.5%),p<0.001]、既往中风[(1%比第二波和第一波分别为 4.1%),p=0.046]。就临床和实验室检查结果而言,我们的研究发现,第一波患者的血红蛋白和 HIV 病毒载量更高。另一方面,第二波患者的胸部 X 线异常、吸入氧分数(FiO2)和尿毒症的发生率明显更高。第一波和第二波之间的死亡与出院的调整比值比相似(0.94,95%CI:0.84-1.05)。第一波的平均存活时间更长(8.0 天比 6.1 天),出院存活患者的平均住院时间更短(9.2 天比 10.7 天)。潜在类别分析显示,心血管表型的死亡率最高,其次是糖尿病和 CKD 表型。只有糖尿病和高血压表型的死亡率最低。
尽管两次波之间的临床和实验室特征存在显著差异,但死亡率保持不变。根据潜在类别分析,心血管、糖尿病和 CKD 表型的死亡概率最高。