From the Department of Radiology, Nottingham University Hospitals National Health Service (NHS) Trust, Nottingham, England (I.A.Y., Y.H., E.G.); Respiratory Medicine (A.F.), Gastroenterology (C.J.C., T.C., J.W.), Department of Critical Care (M.S.), Department of Digital Services (I.J.), Department of Corporate Services (A.R., S.H.P.), Specialist Support Directorate (S.C.), Nottingham University Hospitals NHS Trust, Nottingham, England (J.R.M., S.B.); Translational Medical Sciences, School of Medicine, University of Nottingham, Nottingham, England NG7 2UH (C.J.C.); Population and Lifespan Sciences, School of Medicine, University of Nottingham, Nottingham NG5 1PB, England (A.F., J.R.M., M.G., J.W., T.C.); NIHR Nottingham Biomedical Research Centre (BRC), Nottingham University Hospitals NHS Trust and the University of Nottingham, Nottingham, England (A.F., J.R.M., J.W., C.J.C., T.C.); and East Midlands Academic Health Science Network, University of Nottingham, Nottingham, England (J.W.).
Radiology. 2022 Feb;302(2):460-469. doi: 10.1148/radiol.2021210986. Epub 2021 Sep 14.
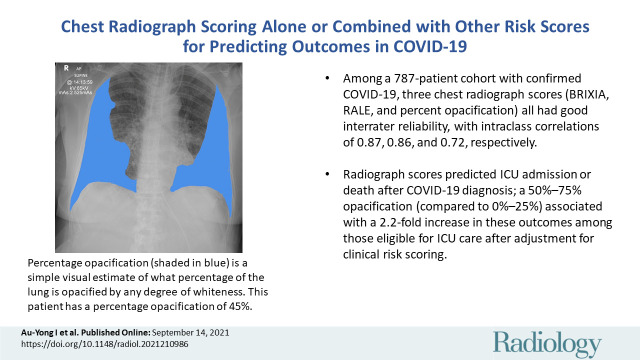
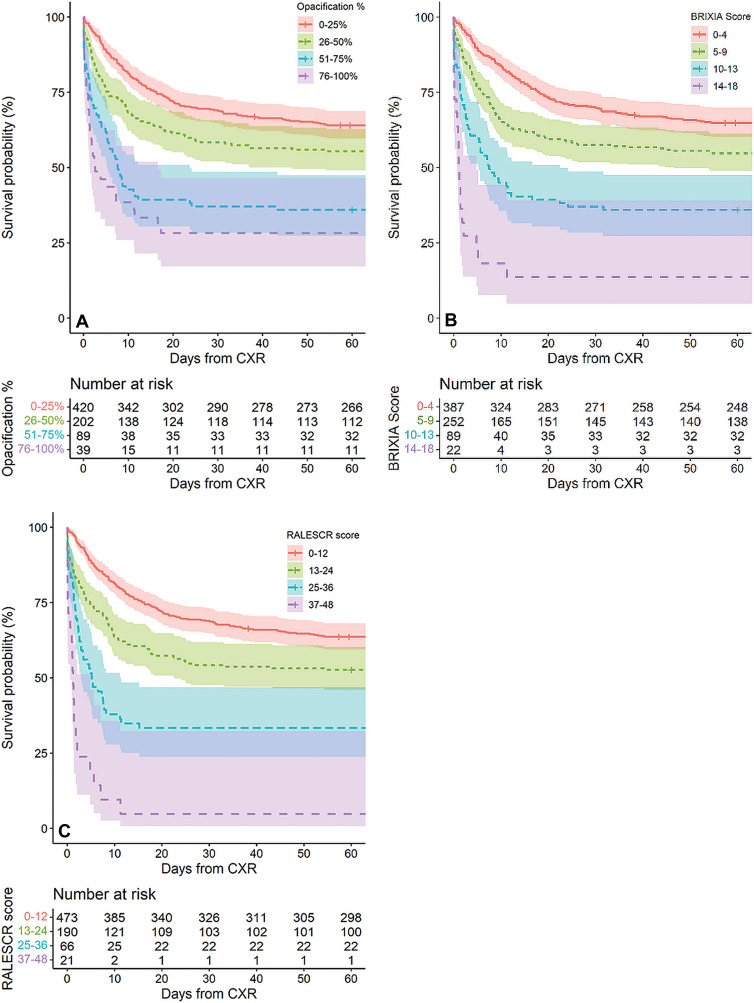
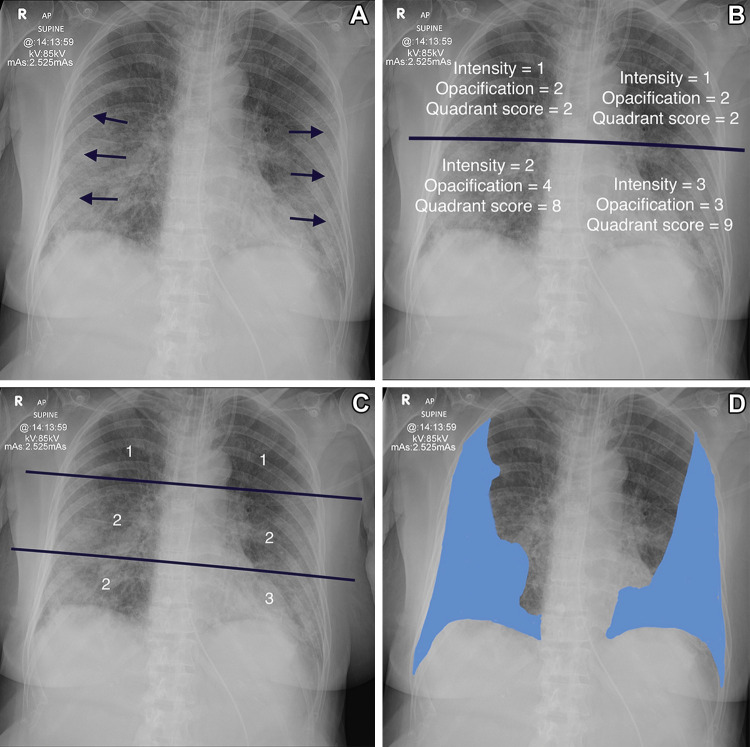
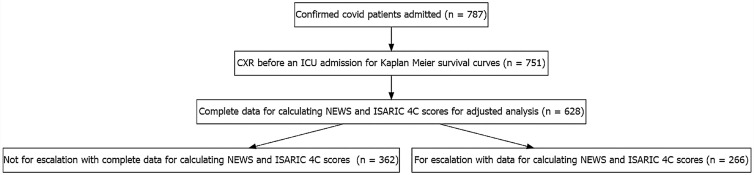
Background Radiographic severity may help predict patient deterioration and outcomes from COVID-19 pneumonia. Purpose To assess the reliability and reproducibility of three chest radiograph reporting systems (radiographic assessment of lung edema [RALE], Brixia, and percentage opacification) in patients with proven SARS-CoV-2 infection and examine the ability of these scores to predict adverse outcomes both alone and in conjunction with two clinical scoring systems, National Early Warning Score 2 (NEWS2) and International Severe Acute Respiratory and Emerging Infection Consortium: Coronavirus Clinical Characterization Consortium (ISARIC-4C) mortality. Materials and Methods This retrospective cohort study used routinely collected clinical data of patients with polymerase chain reaction-positive SARS-CoV-2 infection admitted to a single center from February 2020 through July 2020. Initial chest radiographs were scored for RALE, Brixia, and percentage opacification by one of three radiologists. Intra- and interreader agreement were assessed with intraclass correlation coefficients. The rate of admission to the intensive care unit (ICU) or death up to 60 days after scored chest radiograph was estimated. NEWS2 and ISARIC-4C mortality at hospital admission were calculated. Daily risk for admission to ICU or death was modeled with Cox proportional hazards models that incorporated the chest radiograph scores adjusted for NEWS2 or ISARIC-4C mortality. Results Admission chest radiographs of 50 patients (mean age, 74 years ± 16 [standard deviation]; 28 men) were scored by all three radiologists, with good interreader reliability for all scores, as follows: intraclass correlation coefficients were 0.87 for RALE (95% CI: 0.80, 0.92), 0.86 for Brixia (95% CI: 0.76, 0.92), and 0.72 for percentage opacification (95% CI: 0.48, 0.85). Of 751 patients with a chest radiograph, those with greater than 75% opacification had a median time to ICU admission or death of just 1-2 days. Among 628 patients for whom data were available (median age, 76 years [interquartile range, 61-84 years]; 344 men), opacification of 51%-75% increased risk for ICU admission or death by twofold (hazard ratio, 2.2; 95% CI: 1.6, 2.8), and opacification greater than 75% increased ICU risk by fourfold (hazard ratio, 4.0; 95% CI: 3.4, 4.7) compared with opacification of 0%-25%, when adjusted for NEWS2 score. Conclusion Brixia, radiographic assessment of lung edema, and percentage opacification scores all reliably helped predict adverse outcomes in SARS-CoV-2 infection. © RSNA, 2021 See also the editorial by Little in this issue.
背景 放射学严重程度可能有助于预测 COVID-19 肺炎患者的病情恶化和结局。目的 评估三种胸部 X 线报告系统(肺水肿放射学评估[RALE]、Brixia 和肺不张百分比)在已确诊 SARS-CoV-2 感染患者中的可靠性和可重复性,并检查这些评分单独以及与两个临床评分系统(国家早期预警评分 2 [NEWS2]和国际严重急性呼吸和新兴感染联盟:冠状病毒临床特征联盟[ISARIC-4C]死亡率)联合使用时预测不良结局的能力。材料与方法 这项回顾性队列研究使用了 2020 年 2 月至 7 月期间在一家中心因聚合酶链反应阳性 SARS-CoV-2 感染而入院的患者的常规临床数据。由三位放射科医生之一对初始胸部 X 光片进行 RALE、Brixia 和肺不张百分比评分。采用组内相关系数评估内部和读者间的一致性。根据评分的胸部 X 光片,估计入住重症监护病房(ICU)或死亡的比例在 60 天内。计算入院时的 NEWS2 和 ISARIC-4C 死亡率。使用 Cox 比例风险模型对 ICU 入住或死亡的每日风险进行建模,该模型将胸部 X 光片评分调整为 NEWS2 或 ISARIC-4C 死亡率。结果 50 名患者(平均年龄,74 岁±16[标准差];28 名男性)的入院胸部 X 光片由所有三位放射科医生评分,所有评分的读者间一致性均较好,如下所示:组内相关系数分别为 0.87(95%CI:0.80,0.92)、0.86(95%CI:0.76,0.92)和 0.72(95%CI:0.48,0.85)。在 751 名有胸部 X 光片的患者中,75%以上肺不张的患者入住 ICU 或死亡的中位时间仅为 1-2 天。在 628 名可获得数据的患者中(中位年龄,76 岁[四分位间距,61-84 岁];344 名男性),51%-75%的肺不张使 ICU 入住或死亡的风险增加一倍(危险比,2.2;95%CI:1.6,2.8),而大于 75%的肺不张使 ICU 风险增加四倍(危险比,4.0;95%CI:3.4,4.7)与 0%-25%的肺不张相比,当调整为 NEWS2 评分时。结论 Brixia、肺水肿放射学评估和肺不张百分比评分均可靠地有助于预测 SARS-CoV-2 感染的不良结局。