Institute of Movement and Locomotion, Aix-Marseille Université et CNRS 5, Marseille, France.
CEReSS-Health Services Research and Quality of Life Center, Faculté de Médecine, Secteur Timone, EA 3279, CEReSS -Centre D'Etude Et de Recherche Sur Les Services de Santé Et La Qualité de Vie, Aix-Marseille University, 27 Boulevard Jean Moulin, 13005, Marseille, France.
Sci Rep. 2023 Oct 6;13(1):16849. doi: 10.1038/s41598-023-43790-8.
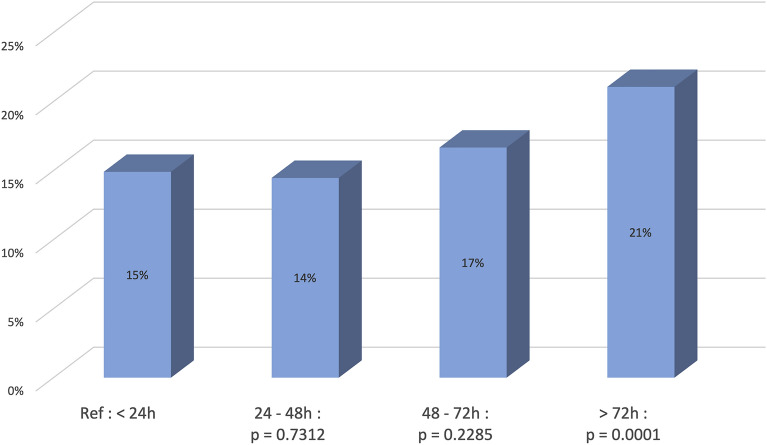
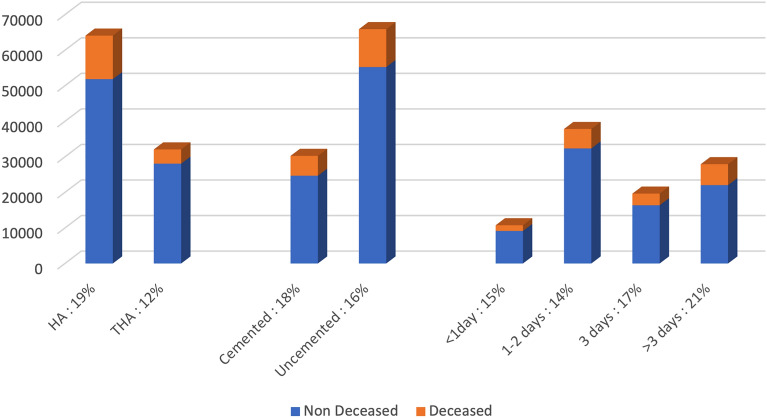
Mortality related to femoral neck fractures remains a challenging health issue, with a high mortality rate at 1 year of follow-up. Three modifiable factors appear to be under control of the surgeon: the choice of the implant, the use of cement and the timing before surgery. The aim of this research project was to study the impact on mortality each of these risk factors play during the management of femoral neck fractures. A large retrospective epidemiological study was performed using a national database of the public healthcare system. The inclusion criteria were patients who underwent joint replacement surgery after femoral neck fracture during the years 2015 to 2017. All data points were available for at least 2 years after the fracture. The primary outcome was mortality within 2 years following the surgery. We evaluated the association between mortality and the type of the implant hemiarthroplasty (HA) versus total hip arthroplasty (THA), cemented versus non cemented femoral stem as well as the timing from fracture to surgical procedure. A multivariate analysis was performed including age, gender, comorbidities/autonomy scores, social category, and obesity. We identified 96,184 patients who matched the inclusion criteria between 2015 and 2017. 64,106 (66%) patients underwent HA and 32,078 (33.4%) underwent THA. After multivariate analysis including age and comorbidities, patients who underwent surgery after 72 h intra-hospital had a higher risk of mortality: Hazard Ratio (HR) = 1.119 (1.056-1.185) p = 0.0001 compared to the group who underwent surgery within 24 h. THA was found to be a protective factor HR = 0.762 (0.731-0.795) p < 0.0001. The use of cement was correlated with higher mortality rate: HR = 1.107 (1.067-1.149) p < 0.0001. Three key points are highlighted by our study in the reduction of mortality related to femoral neck fracture: the use of hemiarthroplasty a surgery performed after 48 h and the use of cement for femoral stem fixation adversely affect mortality risk.
与股骨颈骨折相关的死亡率仍然是一个具有挑战性的健康问题,在随访 1 年后的死亡率很高。有三个可改变的因素似乎在外科医生的控制之下:植入物的选择、使用水泥和手术前的时间。本研究项目的目的是研究这些危险因素在股骨颈骨折管理过程中对死亡率的影响。使用公共医疗保健系统的国家数据库进行了一项大型回顾性流行病学研究。纳入标准为 2015 年至 2017 年期间因股骨颈骨折接受关节置换手术的患者。所有数据点在骨折后至少 2 年都可获得。主要结果是手术后 2 年内的死亡率。我们评估了死亡率与半髋关节置换术(HA)与全髋关节置换术(THA)、骨水泥固定与非骨水泥固定股骨柄之间的关联,以及从骨折到手术的时间。进行了多变量分析,包括年龄、性别、合并症/自主评分、社会类别和肥胖。我们确定了 2015 年至 2017 年期间符合纳入标准的 96184 名患者。64106 名(66%)患者接受 HA,32078 名(33.4%)患者接受 THA。多变量分析包括年龄和合并症后,在医院内 72 小时内进行手术的患者死亡风险更高:风险比(HR)=1.119(1.056-1.185)p=0.0001,与 24 小时内进行手术的患者相比。THA 被发现是一个保护因素 HR=0.762(0.731-0.795)p<0.0001。使用水泥与更高的死亡率相关:HR=1.107(1.067-1.149)p<0.0001。我们的研究强调了三个降低股骨颈骨折相关死亡率的关键点:使用半髋关节置换术、48 小时后进行手术以及使用水泥固定股骨柄会增加死亡率风险。