Sun Rui, Lu Wenli, Ren Wanhua, Zhang Shuhong, Yao Dongxue, Zhang Nannan, Zhong Keqing, Zhao Wenrui, Tang Xiaolin, Han Meihong, Li Tao
Department of Infectious Diseases, Shandong Provincial Hospital, Shandong University, Jinan, China.
Department of Infectious Diseases, Shandong Provincial Hospital Affiliated to Shandong First Medical University, 324#, Jing 5 Road, Jinan, China.
Sci Rep. 2023 Oct 8;13(1):16970. doi: 10.1038/s41598-023-44006-9.
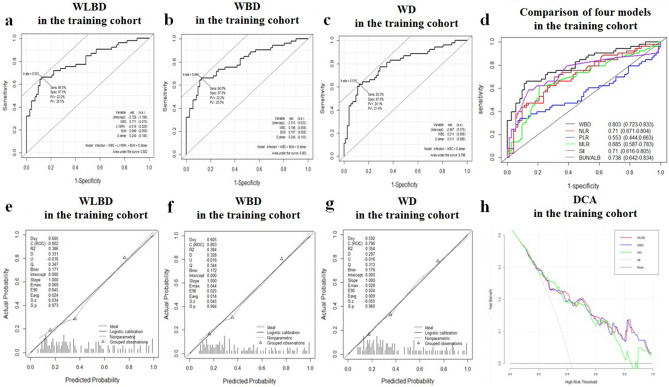
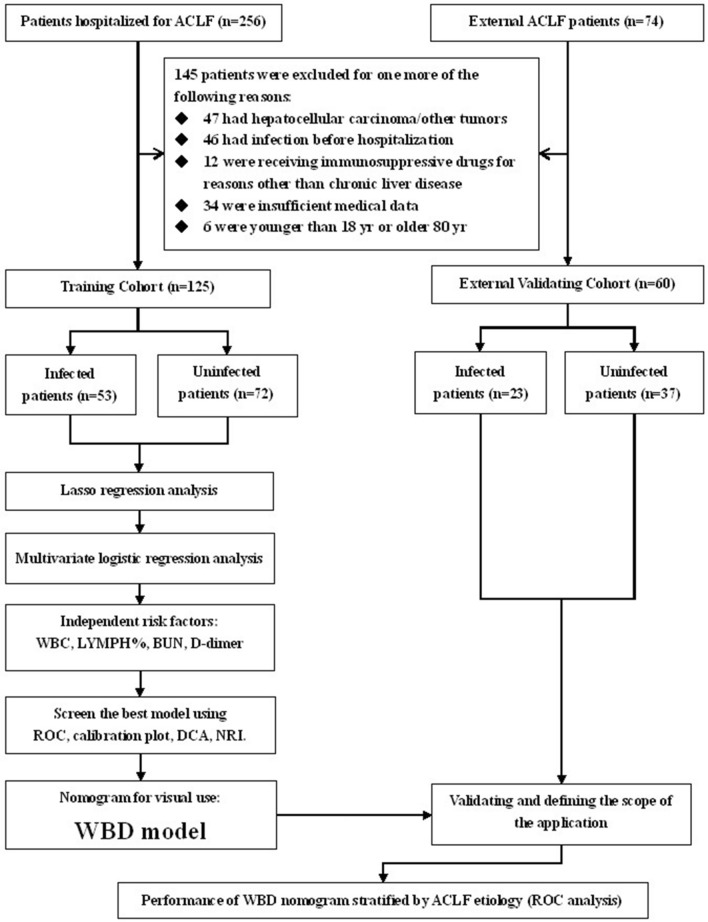
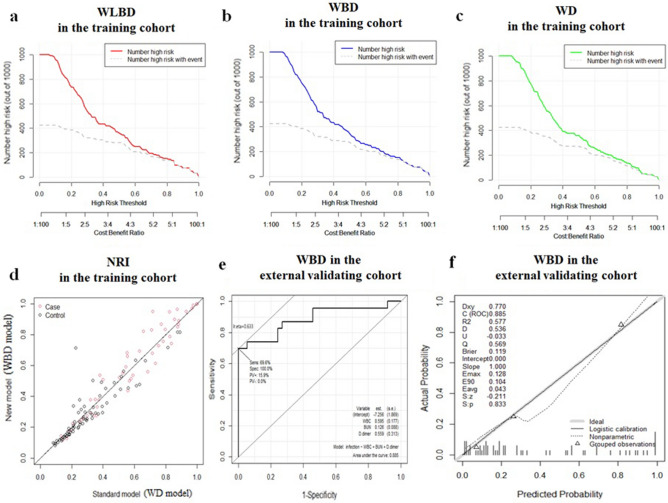
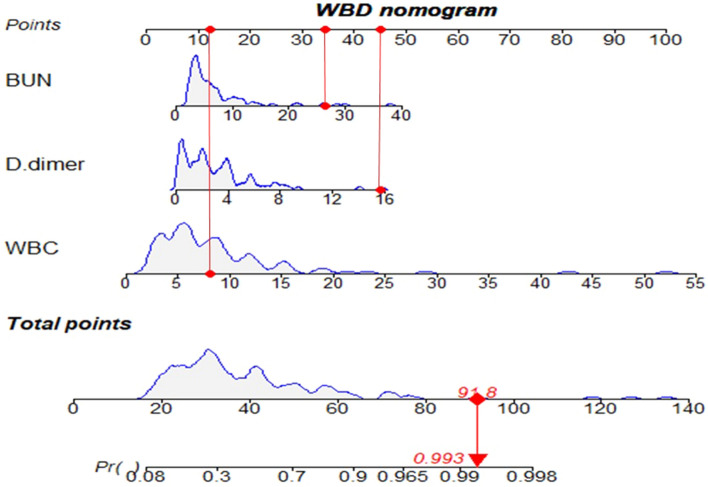
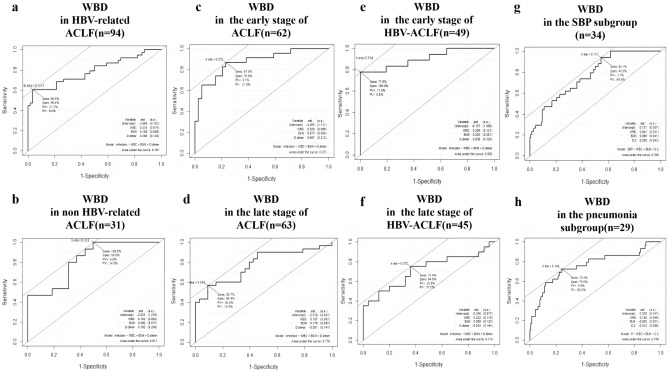
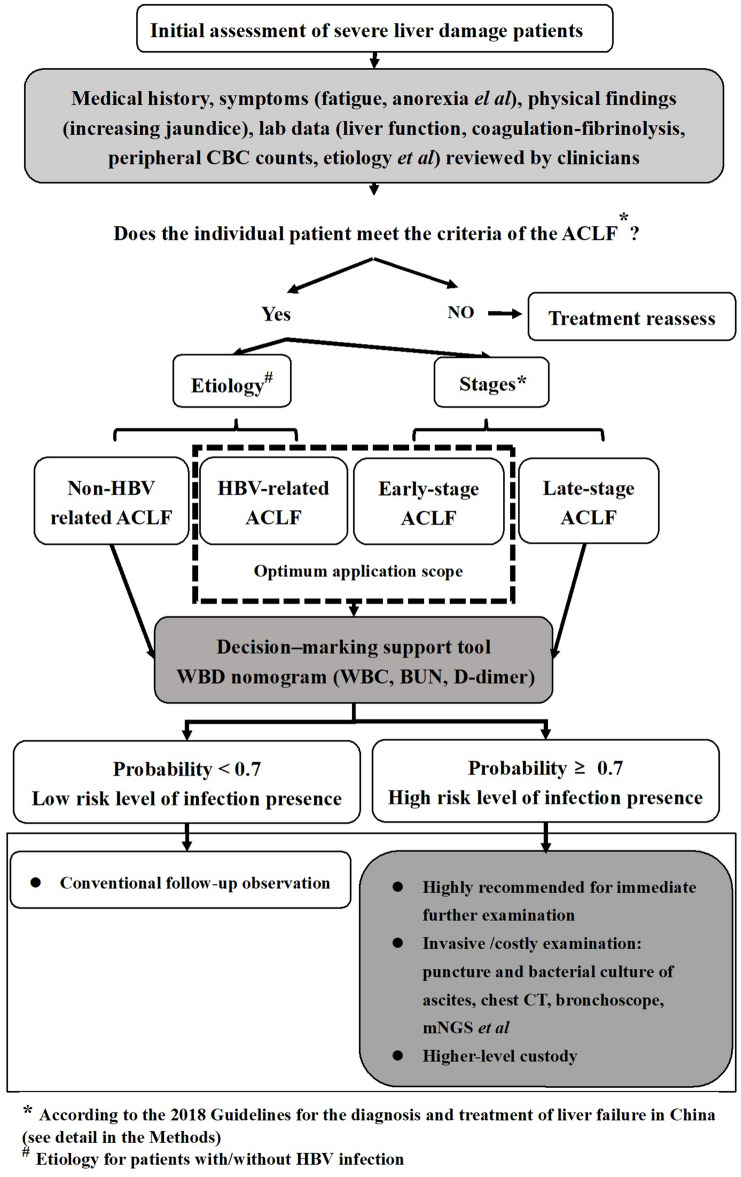
Accurate assessment of infection presence risk level, timely diagnosis, and effective control are critical for decreasing mortality of Acute‑on‑chronic liver failure (ACLF). We aimed to develop and validate a novel diagnostic model to accurately assess infection presence risk level in ACLF patients. 185 ACLF patients with/without infection were enrolled, and their demographic, physical findings, immune-inflammatory, hepatic function, metabolism, and coagulation-fibrinolysis indicators were analyzed. Regression analysis was performed to identify the independent diagnostic parameters, which were further used to establish diagnostic models with a nomogram for visual. An area under receiver operating characteristic curve (AUROC), calibration plots, clinical impact curves, decision curve analysis, and net reclassification index were used to evaluate and identify the best model. An external validating cohort was introduced to verify the diagnostic accuracy. We screened out white blood cell (WBC) count, LYM%, blood urea nitrogen (BUN), and D-dimer for assessing infection presence risk levels in ACLF patients. WBD (WBC + BUN + D-dimer) was established and proposed as a novel diagnostic model for infection presence risk levels assessment in ACLF patients with an AUROC of 0.803 (95%CI 0.723-0.883), 0.885 (95%CI 0.786-0.984) in training and external cohorts, respectively. In stratification analysis by ACLF etiology and stages, WBD achieved an AUROC of 0.791 (95%CI 0.691-0.891) and 0.873 (95%CI 0.78-0.966) in HBV-related and early-stage patients, respectively. Whereas a higher AUROC of 0.905 (95%CI 0.807-1.00) in the early-stage of HBV-related ACLF patients indicated its optimum application scope. WBD, a novel laboratory-based nomogram, can serve as a decision-making support tool for clinicians to assess infection presence risk levels in ACLF patients.
准确评估感染存在风险水平、及时诊断和有效控制对于降低慢加急性肝衰竭(ACLF)的死亡率至关重要。我们旨在开发并验证一种新型诊断模型,以准确评估ACLF患者的感染存在风险水平。纳入了185例有/无感染的ACLF患者,并分析了他们的人口统计学、体格检查结果、免疫炎症、肝功能、代谢及凝血纤溶指标。进行回归分析以确定独立诊断参数,这些参数进一步用于建立带有列线图以便直观显示的诊断模型。采用受试者工作特征曲线下面积(AUROC)、校准图、临床影响曲线、决策曲线分析和净重新分类指数来评估并确定最佳模型。引入外部验证队列以验证诊断准确性。我们筛选出白细胞(WBC)计数、淋巴细胞百分比(LYM%)、血尿素氮(BUN)和D-二聚体用于评估ACLF患者的感染存在风险水平。建立了WBD(WBC+BUN+D-二聚体)并将其作为一种新型诊断模型用于评估ACLF患者的感染存在风险水平,在训练队列和外部队列中的AUROC分别为0.803(95%CI 0.723-0.883)、0.885(95%CI 0.786-0.984)。在按ACLF病因和分期进行的分层分析中,WBD在乙型肝炎病毒(HBV)相关患者和早期患者中分别达到了0.791(95%CI 0.691-0.891)和0.873(95%CI 0.78-0.966)的AUROC。而在HBV相关ACLF患者早期,AUROC高达0.905(95%CI 0.807-1.00),表明了其最佳应用范围。WBD,一种基于实验室的新型列线图,可作为临床医生评估ACLF患者感染存在风险水平的决策支持工具。