Department of Biomedicine & Health Sciences, Graduate School, The Catholic University of Korea, Seoul, Republic of Korea.
Department of Laboratory Medicine, Uijeongbu Paik Hospital, Uijeongbu, Republic of Korea.
Front Immunol. 2023 Sep 21;14:1243912. doi: 10.3389/fimmu.2023.1243912. eCollection 2023.
Polyomavirus (BKV) infection can lead to major complications and damage to the graft in kidney transplant recipients (KTRs). We investigated whether pretransplant BK serostatus and BK-specific cell-mediated immunity (CMI) predicts post-transplant BK infection.
A total of 93 donor-recipient pairs who underwent kidney transplantation (KT) and 44 healthy controls were examined. Assessment of donor and recipient BKV serostatus and BKV-CMI in recipients was performed prior to transplantation using BKV-IgG ELISA and BKV-specific IFN-g ELISPOT assays against five BK viral antigens (LT, St, VP1, VP2, and VP3). BK viremia was diagnosed when blood BKV-DNA of 104 copies/mL or more was detected during follow-up periods.
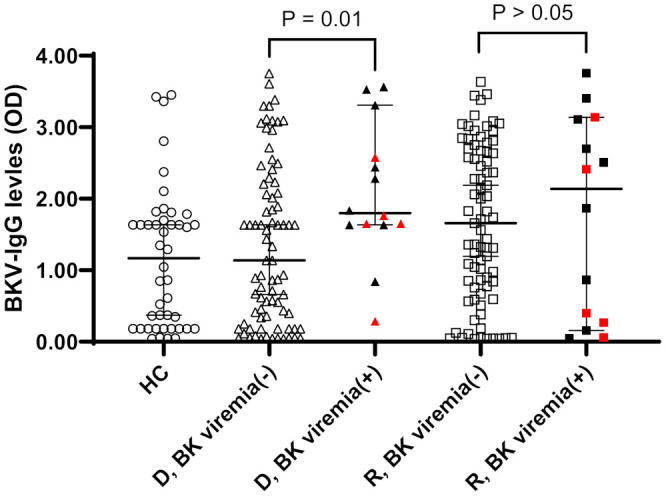
Anti-BKV IgG antibody was detected in 74 (79.6%) of 93 KTRs and in 68 (73.1%) of 93 KT donors. A greater percentage of KTRs who received allograft from donors with high levels of anti-BKV IgG had posttransplant BK viremia (+) than KTRs from donors with low anti-BKV IgG (25.5% [12/47] vs. 4.3% [2/46], respectively; P = 0.007). Pretransplant total BKV-ELISPOT results were lower in BK viremia (+) patients than in patients without viremia (-) 20.5 [range 9.9-63.6] vs. 72.0 [43.2 - 110.8]; P = 0. 027). The sensitivity and specificity of the total BKV-ELISPOT assay (cut-off ≤ 53 spots/3×105 cells) for prediction of posttransplant BK viremia were 71.4 (95% CI: 41.9-91.6) and 54.4 (42.8-65.7), respectively. The combination of high donor BKV-IgG, low recipient BKV-IgG, and low total BKV-ELISPOT results improved specificity to 91.1%.
Our study highlights the importance of pretransplant BKV-IgG serostatus and BKV-specific CMI in predicting posttransplant BKV infection in KTRs. The combination of high donor BKV-IgG, low recipient BKV-IgG, and low total BKV-ELISPOT results predicted BK viremia after KT. Pretransplant identification of patients at highrisk for BK viremia could enable timely interventions and improve clinical outcomes of KTRs.
多瘤病毒(BKV)感染可导致肾移植受者(KTR)的主要并发症和移植物损害。我们研究了移植前 BK 血清状态和 BK 特异性细胞介导免疫(CMI)是否可以预测移植后 BK 感染。
共检查了 93 对接受肾移植(KT)的供体-受体和 44 名健康对照者。在移植前使用 BKV-IgG ELISA 和针对 5 种 BK 病毒抗原(LT、St、VP1、VP2 和 VP3)的 BK 特异性 IFN-γ ELISPOT 测定法评估供体和受体的 BKV 血清状态和受体中的 BKV-CMI。在随访期间检测到血液 BKV-DNA 超过 104 拷贝/mL 时,诊断 BK 病毒血症。
93 名 KTR 中有 74 名(79.6%)和 93 名 KT 供体中有 68 名(73.1%)检测到抗 BKV IgG 抗体。与来自低抗 BKV IgG 供体的 KTR 相比,从高抗 BKV IgG 供体接受同种异体移植物的 KTR 移植后 BK 病毒血症(+)的比例更高(分别为 25.5%[12/47]和 4.3%[2/46];P=0.007)。BK 病毒血症(+)患者的移植前总 BKV-ELISPOT 结果低于无病毒血症(-)患者 20.5[范围 9.9-63.6]与 72.0[43.2-110.8];P=0.027)。总 BKV-ELISPOT 检测(≤53 个斑点/3×105 个细胞)对预测移植后 BK 病毒血症的敏感性和特异性分别为 71.4%(95%CI:41.9-91.6)和 54.4%(42.8-65.7)。高供体 BKV-IgG、低受体 BKV-IgG 和低总 BKV-ELISPOT 结果的组合将特异性提高至 91.1%。
我们的研究强调了移植前 BKV-IgG 血清状态和 BKV 特异性 CMI 在预测 KTR 移植后 BKV 感染中的重要性。高供体 BKV-IgG、低受体 BKV-IgG 和低总 BKV-ELISPOT 结果的组合预测了 KT 后的 BK 病毒血症。在 BK 病毒血症高危患者中,在移植前确定可以及时进行干预并改善 KTR 的临床结果。