Department of Medical Oncology, School of Medicine, Acibadem University, Istanbul, Turkey.
University of California San Francisco, Helen Diller Family Comprehensive Cancer Center, San Francisco, CA, USA.
Breast Cancer Res Treat. 2024 Jan;203(2):197-204. doi: 10.1007/s10549-023-07073-0. Epub 2023 Oct 10.
We hypothesized that eribulin combined with cyclophosphamide (EC) would be an effective combination with tolerable toxicity for the treatment of advanced breast cancer (ABC).
Patients with histologically confirmed metastatic or unresectable ABC with any number of prior lines of therapy were eligible to enroll. In the dose escalation cohort, dose level 0 was defined as eribulin 1.1 mg/m and cyclophosphamide 600 mg/m and dose level 1 was defined as eribulin 1.4 mg/m and cyclophosphamide 600 mg/m. Eribulin was given on days 1 and 8 and cyclophosphamide on day 1 of a 21-day cycle. In the dose expansion cohort, enrollment was expanded at dose level 1. The primary objective was clinical benefit rate (CBR), and secondary objectives were response rate (RR), duration of response (DOR), progression-free survival (PFS), and safety.
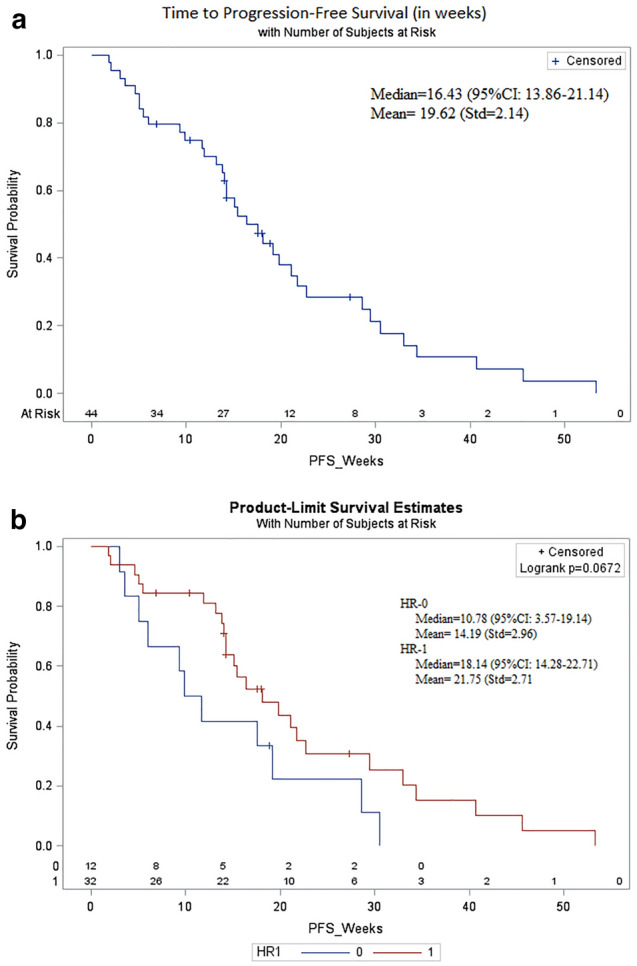
No dose-limiting toxicities were identified in the dose escalation cohort (n = 6). In the dose expansion cohort, an additional 38 patients were enrolled for a total of 44 patients, including 31 patients (70.4%) with hormone receptor-positive (HR +)/HER2- disease, 12 patients (27.3%) with triple-negative breast cancer (TNBC), and 1 patient (2.3%) with HR + /HER2 + disease. Patients had a median age of 56 years (range 33-82 years), 1 prior line of hormone therapy (range 0-6), and 2 prior lines of chemotherapy (range 0-7). CBR was 79.5% (35/44; 7 partial response, 28 stable disease) and the median DOR was 16.4 weeks (range 13.8-21.1 weeks). Median PFS was 16.4 weeks (95% CI: 13.8-21.1 weeks). The most common grade 3/4 adverse event was neutropenia (47.7%, n = 21). Fourteen of 26 patients (53.8%) with circulating tumor cell (CTC) data were CTC-positive ([Formula: see text] 5 CTC/7.5 mL) at baseline. Median PFS was shorter in patients who were CTC-positive vs. negative (13.1 vs 30.6 weeks, p = 0.011).
In heavily pretreated patients with ABC, treatment with EC resulted in an encouraging CBR of 79.5% and PFS of 16.4 weeks, which compares favorably to single-agent eribulin. Dose reduction and delays were primarily due to neutropenia. The contribution of cyclophosphamide to eribulin remains unclear but warrants further evaluation. NCT01554371.
我们假设表柔比星联合环磷酰胺(EC)治疗晚期乳腺癌(ABC)是一种有效且毒性可耐受的联合治疗方法。
本研究纳入了组织学确诊的转移性或不可切除的 ABC 患者,且患者既往接受过任意线数的治疗。在剂量递增队列中,定义剂量 0 为表柔比星 1.1mg/m2 和环磷酰胺 600mg/m2,剂量 1 为表柔比星 1.4mg/m2 和环磷酰胺 600mg/m2。表柔比星于第 1 天和第 8 天给药,环磷酰胺于 21 天周期的第 1 天给药。在剂量扩展队列中,在剂量 1 水平上扩大了入组人数。主要终点为临床获益率(CBR),次要终点为缓解率(RR)、缓解持续时间(DOR)、无进展生存期(PFS)和安全性。
在剂量递增队列中未发现剂量限制毒性(n=6)。在剂量扩展队列中,又入组了 38 例患者,总计 44 例患者,包括 31 例(70.4%)激素受体阳性(HR+)/HER2-疾病、12 例(27.3%)三阴性乳腺癌(TNBC)和 1 例(2.3%)HR+/HER2+疾病。患者的中位年龄为 56 岁(范围 33-82 岁),既往接受过 1 线激素治疗(范围 0-6),接受过 2 线化疗(范围 0-7)。CBR 为 79.5%(35/44;7 例部分缓解,28 例疾病稳定),中位 DOR 为 16.4 周(范围 13.8-21.1 周)。中位 PFS 为 16.4 周(95%CI:13.8-21.1 周)。最常见的 3/4 级不良事件是中性粒细胞减少(47.7%,n=21)。26 例有循环肿瘤细胞(CTC)数据的患者中,有 14 例(53.8%)基线时 CTC 阳性([Formula: see text]5 CTC/7.5mL)。CTC 阳性患者的中位 PFS 短于 CTC 阴性患者(13.1 与 30.6 周,p=0.011)。
在既往接受过大量治疗的 ABC 患者中,EC 治疗的 CBR 为 79.5%,PFS 为 16.4 周,与单药表柔比星相比,这一结果令人鼓舞。剂量减少和延迟主要是由于中性粒细胞减少。环磷酰胺对表柔比星的作用尚不清楚,但值得进一步评估。NCT01554371。