Department of Health Research Methods, Evidence, and Impact, McMaster University, Hamilton, Canada.
Department of Anesthesia, McMaster University, Hamilton, Canada.
JAMA Netw Open. 2023 Oct 2;6(10):e2337239. doi: 10.1001/jamanetworkopen.2023.37239.
Postoperative delirium (POD) is a common and serious complication after surgery. Various predisposing factors are associated with POD, but their magnitude and importance using an individual patient data (IPD) meta-analysis have not been assessed.
To identify perioperative factors associated with POD and assess their relative prognostic value among adults undergoing noncardiac surgery.
MEDLINE, EMBASE, and CINAHL from inception to May 2020.
Studies were included that (1) enrolled adult patients undergoing noncardiac surgery, (2) assessed perioperative risk factors for POD, and (3) measured the incidence of delirium (measured using a validated approach). Data were analyzed in 2020.
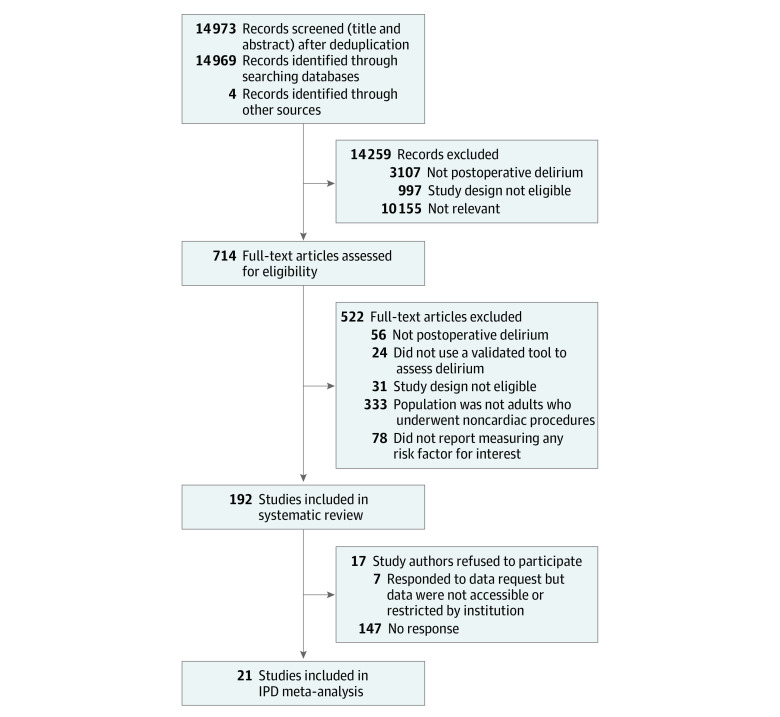
Individual patient data were pooled from 21 studies and 1-stage meta-analysis was performed using multilevel mixed-effects logistic regression after a multivariable imputation via chained equations model to impute missing data.
The end point of interest was POD diagnosed up to 10 days after a procedure. A wide range of perioperative risk factors was considered as potentially associated with POD.
A total of 192 studies met the eligibility criteria, and IPD were acquired from 21 studies that enrolled 8382 patients. Almost 1 in 5 patients developed POD (18%), and an increased risk of POD was associated with American Society of Anesthesiologists (ASA) status 4 (odds ratio [OR], 2.43; 95% CI, 1.42-4.14), older age (OR for 65-85 years, 2.67; 95% CI, 2.16-3.29; OR for >85 years, 6.24; 95% CI, 4.65-8.37), low body mass index (OR for body mass index <18.5, 2.25; 95% CI, 1.64-3.09), history of delirium (OR, 3.9; 95% CI, 2.69-5.66), preoperative cognitive impairment (OR, 3.99; 95% CI, 2.94-5.43), and preoperative C-reactive protein levels (OR for 5-10 mg/dL, 2.35; 95% CI, 1.59-3.50; OR for >10 mg/dL, 3.56; 95% CI, 2.46-5.17). Completing a college degree or higher was associated with a decreased likelihood of developing POD (OR 0.45; 95% CI, 0.28-0.72).
In this systematic review and meta-analysis of individual patient data, several important factors associated with POD were found that may help identify patients at high risk and may have utility in clinical practice to inform patients and caregivers about the expected risk of developing delirium after surgery. Future studies should explore strategies to reduce delirium after surgery.
术后谵妄(POD)是手术后常见且严重的并发症。各种易患因素与 POD 相关,但尚未使用个体患者数据(IPD)荟萃分析评估其严重程度和重要性。
确定与 POD 相关的围手术期因素,并评估其在非心脏手术成年患者中的相对预后价值。
从建库至 2020 年 5 月,检索 MEDLINE、EMBASE 和 CINAHL 数据库。
纳入的研究需(1)纳入接受非心脏手术的成年患者,(2)评估围手术期 POD 的风险因素,以及(3)使用经验证的方法测量谵妄的发生率(采用经验证的方法测量)。数据分析于 2020 年进行。
对 21 项研究中的个体患者数据进行汇总,采用多级混合效应逻辑回归进行 1 阶段荟萃分析,在使用连锁方程模型进行多变量插补后对缺失数据进行插补。
研究的主要结局为术后 10 天内诊断出的 POD。研究考虑了多种围手术期风险因素,这些因素可能与 POD 相关。
共有 192 项研究符合纳入标准,21 项研究获得了 IPD,共纳入 8382 例患者。近 1/5 的患者发生 POD(18%),POD 风险增加与美国麻醉医师协会(ASA)分级 4 相关(比值比[OR],2.43;95%CI,1.42-4.14)、年龄较大(65-85 岁者 OR,2.67;95%CI,2.16-3.29;>85 岁者 OR,6.24;95%CI,4.65-8.37)、低体重指数(体重指数<18.5 者 OR,2.25;95%CI,1.64-3.09)、谵妄病史(OR,3.9;95%CI,2.69-5.66)、术前认知障碍(OR,3.99;95%CI,2.94-5.43)和术前 C 反应蛋白水平(5-10 mg/dL 者 OR,2.35;95%CI,1.59-3.50;>10 mg/dL 者 OR,3.56;95%CI,2.46-5.17)。完成大学学业或以上者发生 POD 的可能性降低(OR,0.45;95%CI,0.28-0.72)。
在这项对个体患者数据的系统评价和荟萃分析中,发现了与 POD 相关的几个重要因素,这些因素可能有助于识别高风险患者,并可能有助于临床实践,以便向患者和护理人员告知手术后发生谵妄的预期风险。未来的研究应探讨降低手术后谵妄的策略。