Department of Intensive Care, Austin Hospital, Melbourne, VIC, Australia.
Australian and New Zealand Intensive Care Research Centre (ANZIC-RC), School of Public Health and Preventive Medicine, Monash University, Melbourne, Australia.
Crit Care. 2023 Oct 12;27(1):371. doi: 10.1186/s13054-023-04644-x.
Mega-dose sodium ascorbate (NaAscorbate) appears beneficial in experimental sepsis. However, its physiological effects in patients with septic shock are unknown.
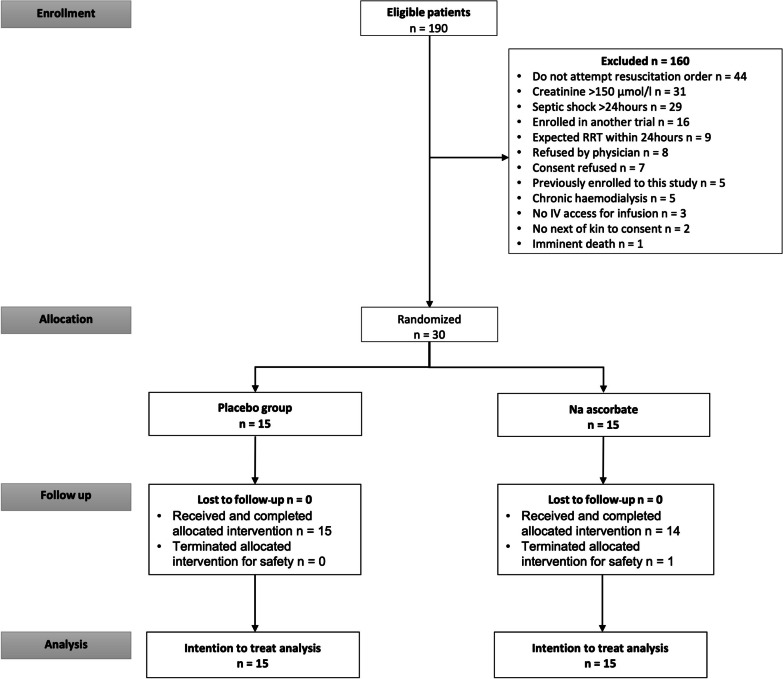
We conducted a pilot, single-dose, double-blind, randomized controlled trial. We enrolled patients with septic shock within 24 h of diagnosis. We randomly assigned them to receive a single mega-dose of NaAscorbate (30 g over 1 h followed by 30 g over 5 h) or placebo (vehicle). The primary outcome was the total 24 h urine output (UO) from the beginning of the study treatment. Secondary outcomes included the time course of the progressive cumulative UO, vasopressor dose, and sequential organ failure assessment (SOFA) score.
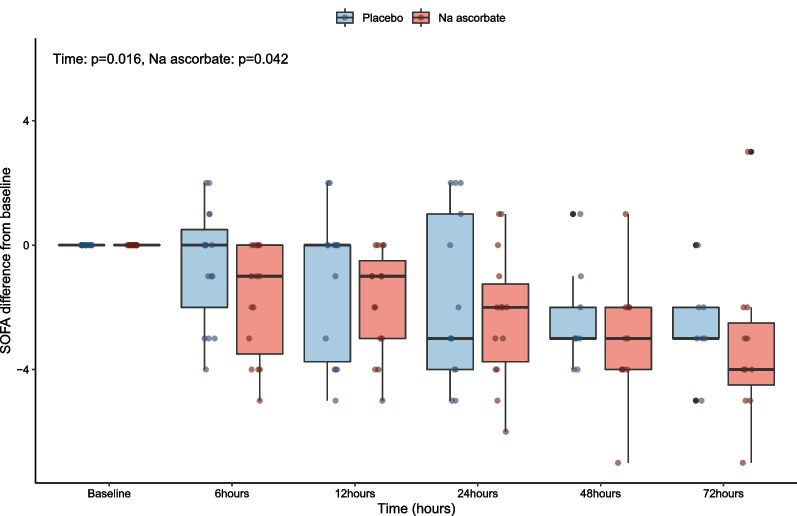
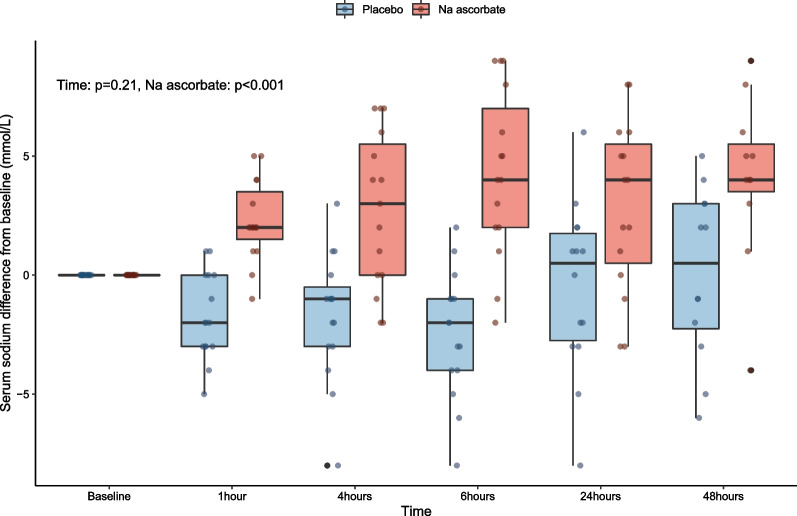
We enrolled 30 patients (15 patients in each arm). The mean (95% confidence interval) total 24-h UO was 2056 (1520-2593) ml with placebo and 2948 (2181-3715) ml with NaAscorbate (mean difference 891.5, 95% confidence interval [- 2.1 to 1785.2], P = 0.051). Moreover, the progressive cumulative UO was greater over time on linear mixed modelling with NaAscorbate (P < 0.001). Vasopressor dose and SOFA score changes over time showed faster reductions with NaAscorbate (P < 0.001 and P = 0.042). The sodium level, however, increased more over time with NaAscorbate (P < 0.001). There was no statistical difference in other clinical outcomes.
In patients with septic shock, mega-dose NaAscorbate did not significantly increase cumulative 24-h UO. However, it induced a significantly greater increase in UO and a greater reduction in vasopressor dose and SOFA score over time. One episode of hypernatremia and one of hemolysis were observed in the NaAscorbate group. These findings support further cautious investigation of this novel intervention. Trial registration Australian New Zealand Clinical Trial Registry (ACTRN12620000651987), Date registered June/5/2020.
大剂量的抗坏血酸钠(NaAscorbate)在实验性败血症中似乎有益。然而,其在感染性休克患者中的生理效应尚不清楚。
我们进行了一项单剂量、双盲、随机对照试验的初步研究。我们招募了在诊断后 24 小时内患有感染性休克的患者。我们将他们随机分配接受单次大剂量的 NaAscorbate(1 小时内输注 30g,然后 5 小时内输注 30g)或安慰剂(载体)。主要结局是从研究治疗开始时的 24 小时总尿量(UO)。次要结局包括渐进性累积 UO、血管加压药剂量和序贯器官衰竭评估(SOFA)评分的时间过程。
我们共纳入了 30 名患者(每组 15 名患者)。安慰剂组 24 小时总尿量为 2056(1520-2593)ml,NaAscorbate 组为 2948(2181-3715)ml(平均差异 891.5,95%置信区间[-2.1 至 1785.2],P=0.051)。此外,线性混合模型显示,随着时间的推移,NaAscorbate 组的渐进性累积 UO 增加更大(P<0.001)。随着时间的推移,血管加压药剂量和 SOFA 评分的变化显示 NaAscorbate 组更快降低(P<0.001 和 P=0.042)。然而,随着时间的推移,NaAscorbate 组的钠离子水平增加更多(P<0.001)。其他临床结局无统计学差异。
在感染性休克患者中,大剂量的 NaAscorbate 并没有显著增加 24 小时累积 UO。然而,它随着时间的推移,导致 UO 显著增加,血管加压药剂量和 SOFA 评分显著降低。NaAscorbate 组出现 1 例高钠血症和 1 例溶血性贫血事件。这些发现支持对这种新干预措施进行进一步谨慎的研究。
澳大利亚和新西兰临床试验注册中心(ACTRN12620000651987),注册日期:2020 年 6 月 5 日。