Gunawardene Melanie A, Frommeyer Gerrit, Ellermann Christian, Jularic Mario, Leitz Patrick, Hartmann Jens, Lange Philipp Sebastian, Anwar Omar, Rath Benjamin, Wahedi Rahin, Eckardt Lars, Willems Stephan
Department of Cardiology and Intensive Care Medicine, Asklepios Hospital St. Georg, 20099 Hamburg, Germany.
Semmelweis University, 1082 Budapest, Hungary.
J Clin Med. 2023 Sep 29;12(19):6304. doi: 10.3390/jcm12196304.
Left atrial posterior wall isolation (LAPWI) may improve rhythm control in addition to pulmonary vein isolation (PVI) in persistent atrial fibrillation (persAF) patients undergoing catheter ablation (CA). However, LAPWI may be challenging when using thermal energy sources.
This study aimed to investigate the efficacy and safety of LAPWI performed by non-thermal pulsed field ablation (PFA) in CA for persAF.
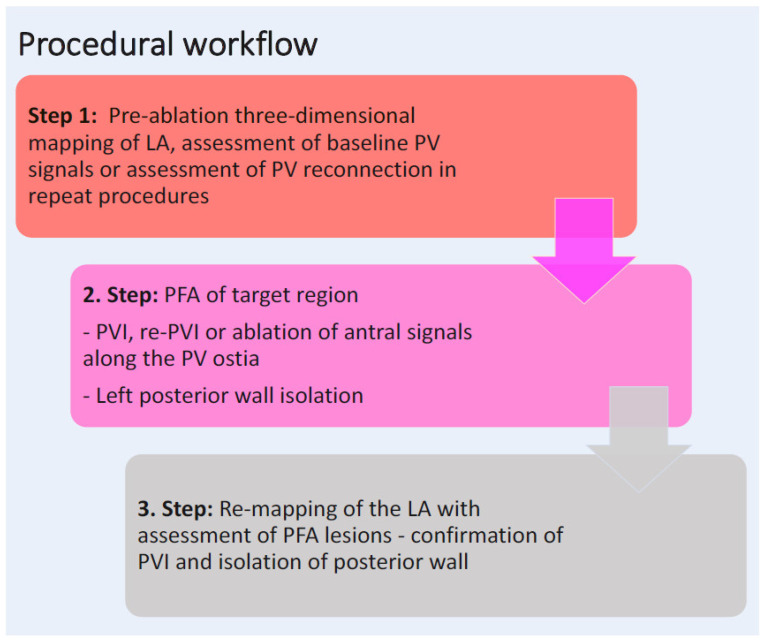
Consecutive persAF patients from two German centers were prospectively enrolled. There were two study cohorts: (1) the LAPWI cohort, which included PFA-guided (re-)PVI with LAPWI for first-time and/or repeat ablation procedures; and (2) a comparative persAF cohort with a PFA PVI-only approach without LAPWI for first-time ablation within the same timeframe. Patients were followed up by routine Holter ECGs.
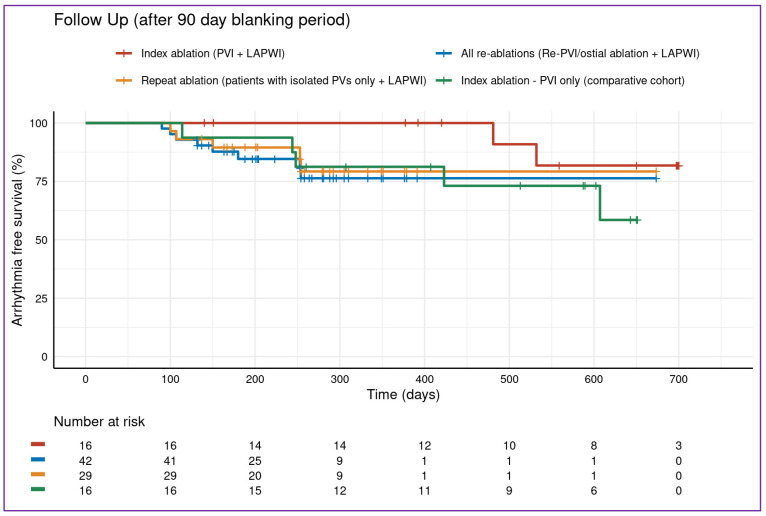
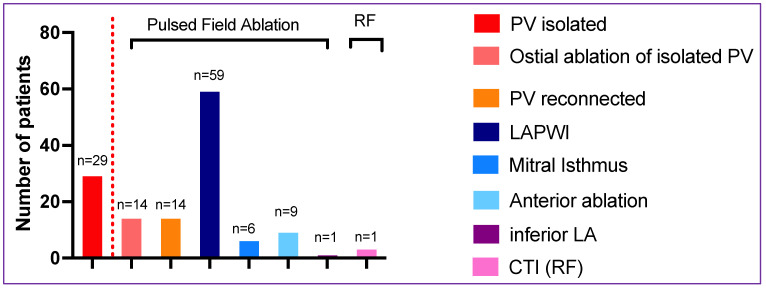
In total, 79 persistent AF patients were included in the study: 59/79 patients were enrolled in the LAPWI cohort, including 16/59 index (27%) and 43/59 repeat ablation procedures (73%). Sixteen patients (16/79; 21%) were in the PVI-only cohort without LAPWI. Of the patients treated with LAPWI, procedure time and fluoroscopy time was 91 ± 30 min and 15 ± 7 min, respectively. The acute PVI rate was 100% in all first-time ablation patients (32 patients (16 PVI only, 16 PVI plus LAPWI), 196/196 PVs). Of the 43 re-do patients in the LAPWI cohort, re-PVI was necessary in 33% (14/43) of patients (27 PVs; 1.9 PV per-patient); in 67% (29/43), all PVs were isolated, and antral ablation of the PV ostia was performed in 48% (14/29). LAPWI was performed successfully in all 59 (100%) patients of the LAPWI cohort. Two minor complications occurred. No esophageal lesion was detected in the LAPWI cohort (n = 33/59 (56%) patients underwent endoscopy). After 354 ± 197 days of follow-up, freedom from atrial arrhythmias was 79.3% (95-CI: 62-95%) in the complete LAPWI cohort (n = 14/59 (24%) on AAD: class Ic n = 9, class III n = 5). There was no difference regarding acute procedural and clinical outcome compared to the PVI-only cohort.
LAPWI guided by PFA is feasible and safe in patients undergoing CA for persAF and shows favorable outcomes. In the context of durable PVI, PFA-guided LAPWI may be an effective adjunctive treatment option.
在接受导管消融(CA)的持续性心房颤动(persAF)患者中,除肺静脉隔离(PVI)外,左心房后壁隔离(LAPWI)可能改善节律控制。然而,使用热能源时LAPWI可能具有挑战性。
本研究旨在探讨非热脉冲场消融(PFA)进行LAPWI在CA治疗persAF中的疗效和安全性。
前瞻性纳入来自两个德国中心的连续persAF患者。有两个研究队列:(1)LAPWI队列,包括首次和/或重复消融手术中PFA引导的(再次)PVI联合LAPWI;(2)一个对比性persAF队列,在同一时间范围内采用仅PFA PVI方法且不进行LAPWI的首次消融。通过常规动态心电图对患者进行随访。
本研究共纳入79例持续性房颤患者:59/79例患者纳入LAPWI队列,包括16/59例初次(27%)和43/59例重复消融手术(73%)。16例患者(16/79;21%)在仅PVI队列中未进行LAPWI。在接受LAPWI治疗的患者中,手术时间和透视时间分别为91±30分钟和15±7分钟。所有初次消融患者(32例患者(16例仅PVI,16例PVI加LAPWI),196/196根肺静脉)的急性PVI成功率为100%。在LAPWI队列的43例再次消融患者中,33%(14/43)的患者需要再次PVI(27根肺静脉;每位患者1.9根肺静脉);67%(29/43)的患者所有肺静脉均被隔离,48%(14/29)的患者进行了肺静脉口部的心房消融。LAPWI队列的所有59例(100%)患者均成功进行了LAPWI。发生了2例轻微并发症。LAPWI队列中未检测到食管病变(n = 33/59(56%)的患者接受了内镜检查)。经过354±197天的随访,整个LAPWI队列(n = 14/59(24%)使用抗心律失常药物:Ic类n = 9,III类n = 5)的无房性心律失常率为79.3%(95%置信区间:62 - 95%)。与仅PVI队列相比,急性手术和临床结果无差异。
PFA引导的LAPWI在接受CA治疗persAF的患者中是可行且安全的,并显示出良好的结果。在持久PVI的背景下,PFA引导的LAPWI可能是一种有效的辅助治疗选择。