Department of Family Medicine and Primary Care, Li Ka Shing Faculty of Medicine, University of Hong Kong, Hong Kong Special Administrative Region (SAR).
Department of Family Medicine and Primary Care, Li Ka Shing Faculty of Medicine, University of Hong Kong, Hong Kong SAR; Department of Family Medicine, University of Hong Kong, Shenzhen Hospital, Shenzhen.
Br J Gen Pract. 2023 Oct 26;73(736):e807-e815. doi: 10.3399/BJGP.2023.0150. Print 2023 Nov.
Continuity of care (COC) is associated with improved health outcomes in patients with hypertension. Team-based COC allows more flexibility in service delivery but there is a lack of research on its effectiveness for patients with hypertension.
To investigate the effectiveness of team-based COC on the prevention of cardiovascular disease (CVD) and mortality in patients with hypertension.
A retrospective cohort study in a primary care setting in Hong Kong.
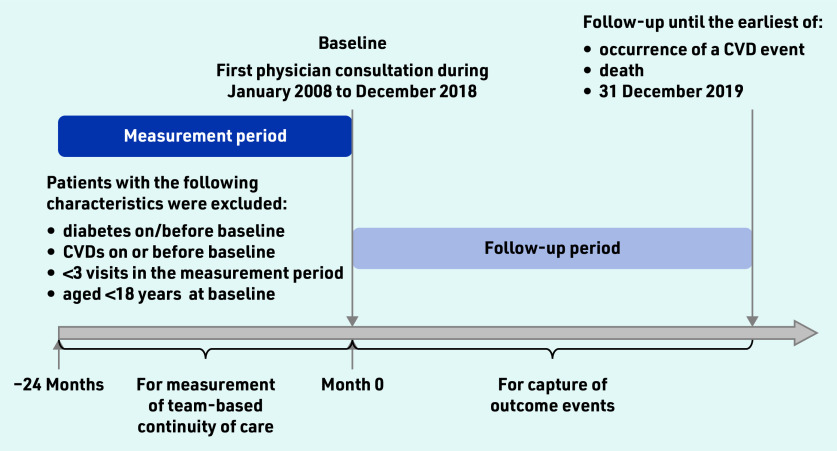
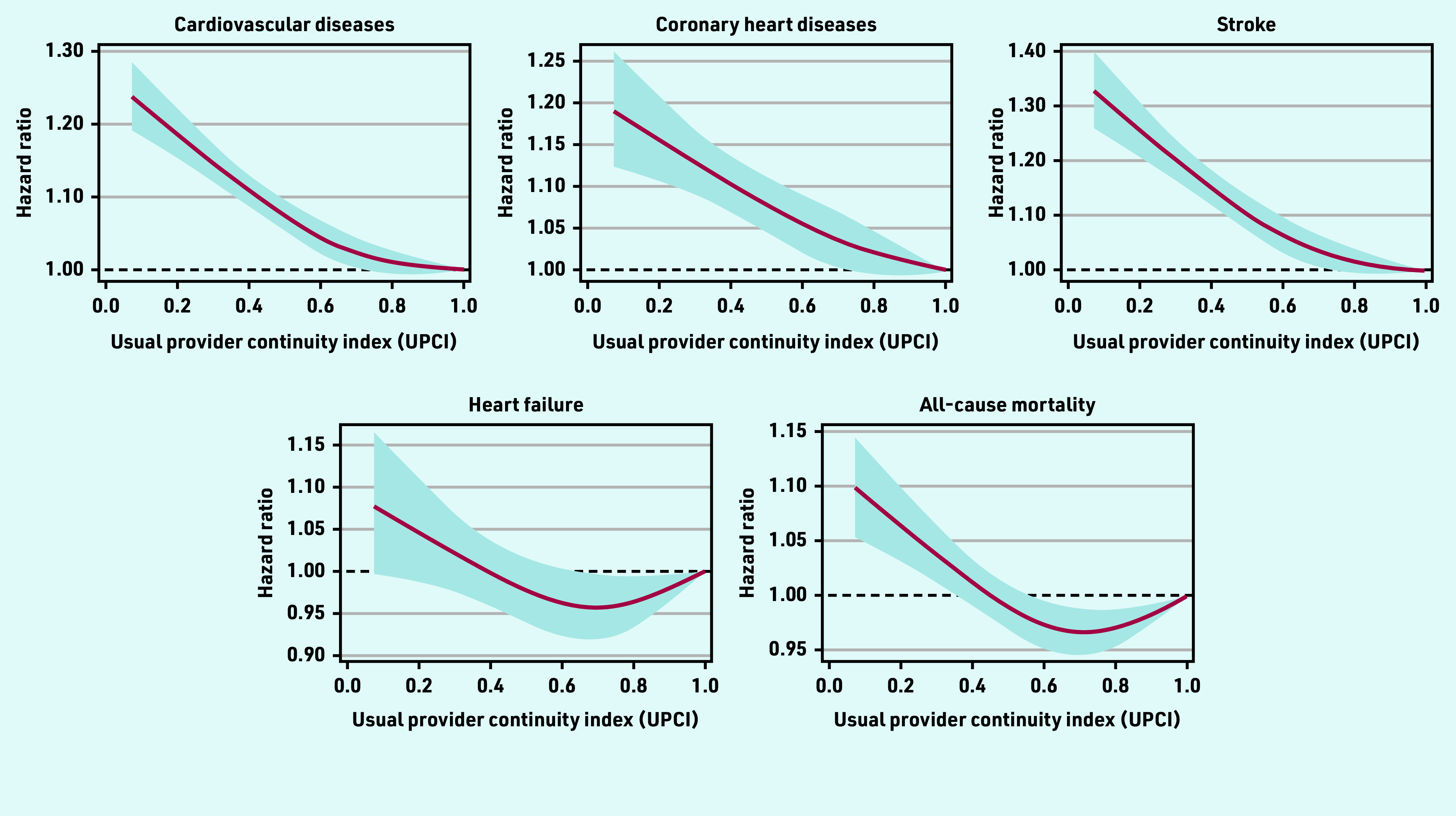
Eligible patients included those visiting public primary care clinics in Hong Kong from 2008 to 2018. The usual provider continuity index (UPCI) was used to measure the COC provided by the most visited physician team. Cox regression and restricted cubic splines were applied to model the association between the COC and the risk for CVDs and all-cause mortality.
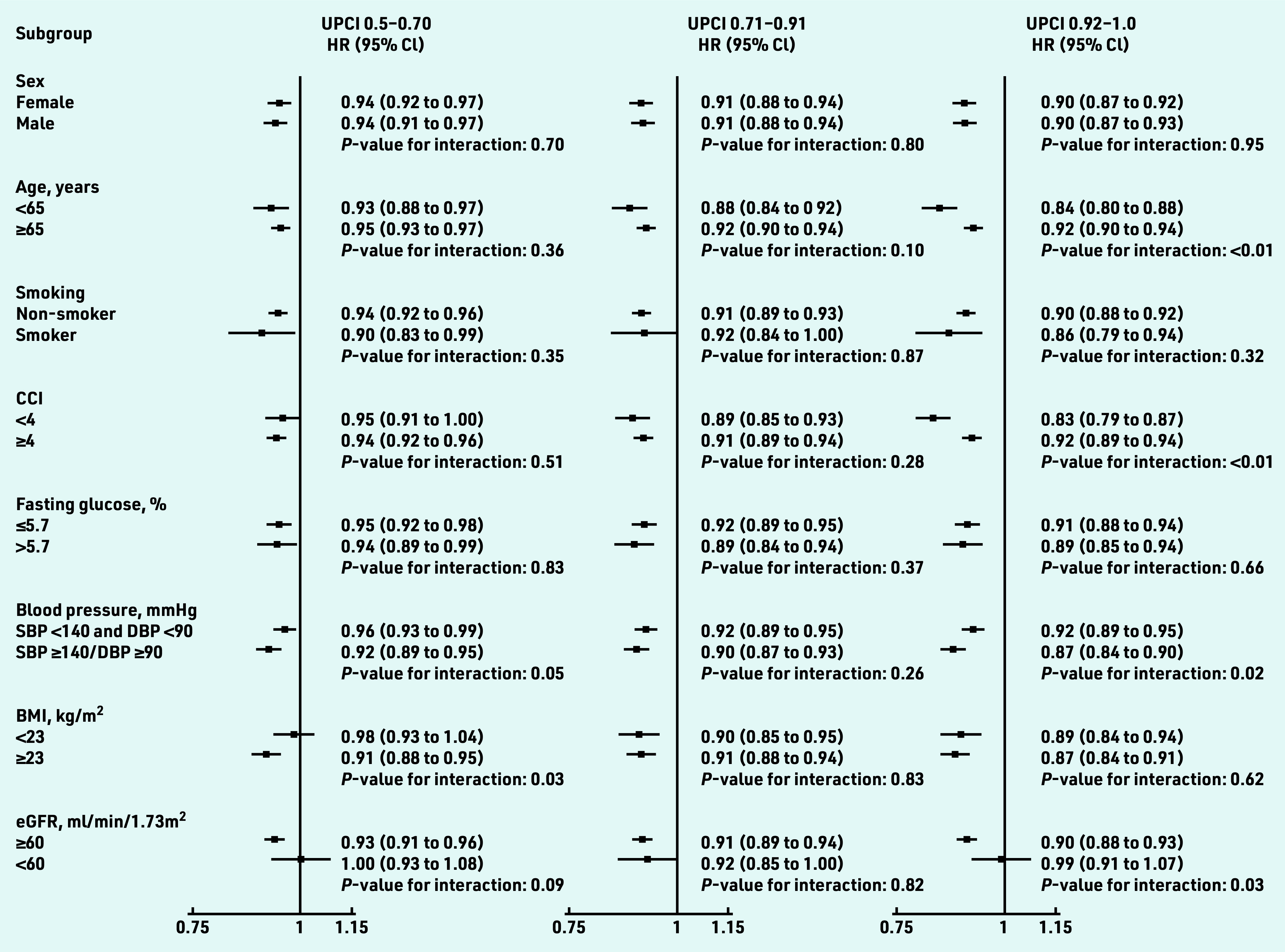
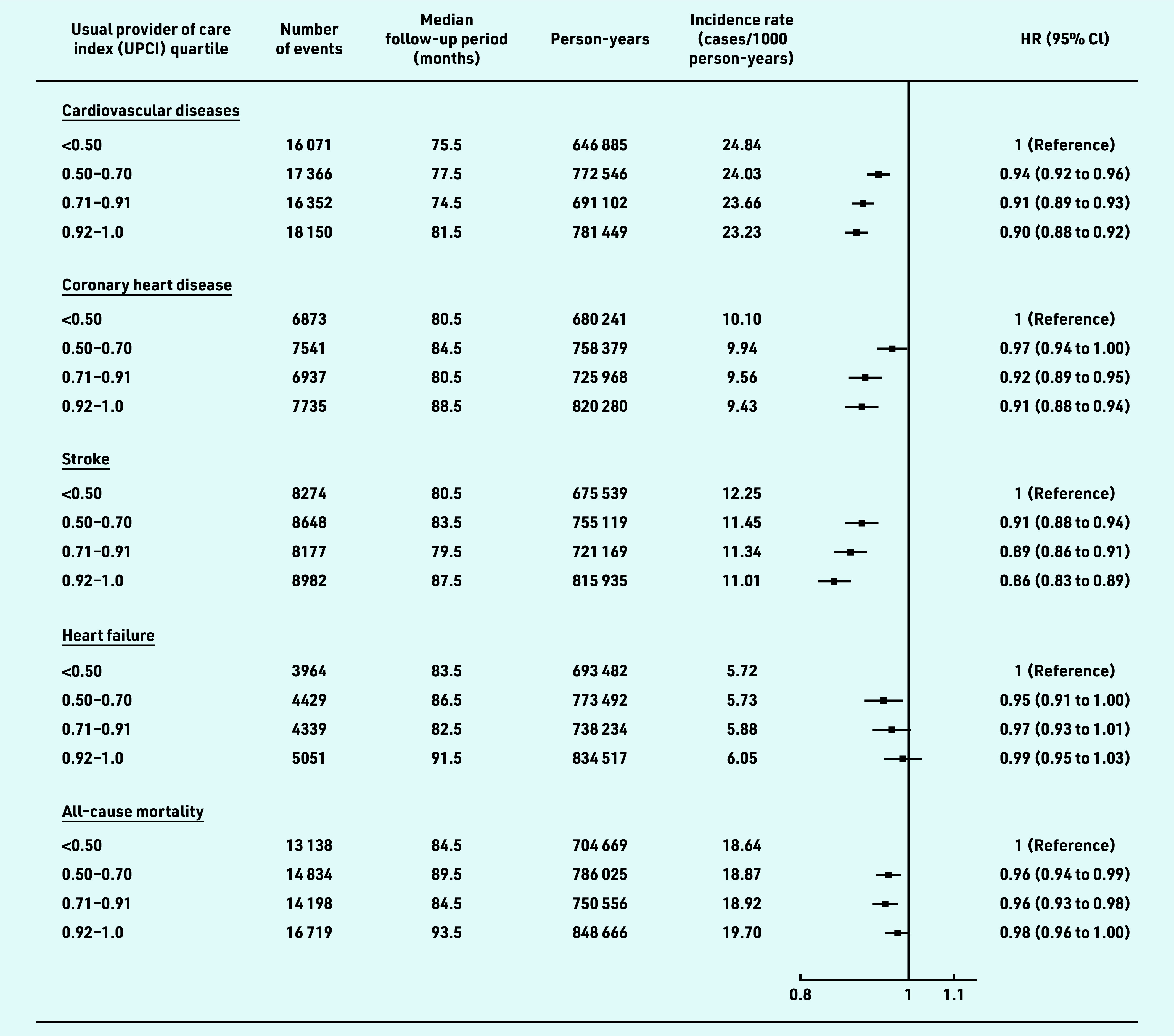
This study included 421 640 eligible patients. Compared with participants in the lowest quartile of UPCI, the hazard ratios for overall CVD were 0.94 (95% CI = 0.92 to 0.96), 0.91(95% CI = 0.89 to 0.93), and 0.90 (95% CI = 0.88 to 0.92) in the second, third, and fourth quartiles, respectively. A greater effect size on CVD risk reduction was observed among the patients with unsatisfactory blood pressure control, patients aged <65 years, and those with a Charlson comorbidity index of <4 at baseline (interaction<0.05 in these subgroup analyses), but the effect was insignificant among the participants with an estimated glomerular filtration rate of <60 ml/ min/1.73 m at baseline.
Team-based COC via a coordinated physician team was associated with reduced risks of CVD and all-cause mortality among patients with hypertension, especially for the patients with unsatisfactory blood pressure control. Early initiation of team-based COC may also achieve extra benefits.
连续性护理(COC)与高血压患者的健康结果改善相关。基于团队的 COC 允许在服务提供方面更具灵活性,但对于高血压患者,其有效性缺乏研究。
调查基于团队的 COC 对预防高血压患者心血管疾病(CVD)和死亡的效果。
在香港基层医疗环境中进行的回顾性队列研究。
纳入的合格患者包括 2008 年至 2018 年期间在香港公共基层医疗诊所就诊的患者。使用最常就诊医生团队的常用提供者连续性指数(UPCI)来衡量 COC。应用 Cox 回归和限制立方样条来构建 UPCI 与 CVD 和全因死亡率风险之间的关联模型。
这项研究纳入了 421640 名合格患者。与 UPCI 最低四分位数的参与者相比,UPCI 第二、三、四分位数的总体 CVD 风险比分别为 0.94(95%CI=0.92 至 0.96)、0.91(95%CI=0.89 至 0.93)和 0.90(95%CI=0.88 至 0.92)。在血压控制不理想、年龄<65 岁以及基线时Charlson 合并症指数<4 的患者中,观察到对 CVD 风险降低的更大效果,而在基线时肾小球滤过率估计值<60ml/min/1.73m2 的患者中,这种效果不显著(这些亚组分析中的交互作用<0.05)。
通过协调医生团队的基于团队的 COC 与高血压患者 CVD 和全因死亡率的风险降低相关,尤其是对于血压控制不理想的患者。早期启动基于团队的 COC 可能还会带来额外的益处。