Department of Interdisciplinary Medicine, University of Bari "Aldo Moro", Piazza Giulio Cesare n. 11, 70124, Bari, Italy.
Center for Outcomes Research and Clinical Epidemiology (CORESEARCH), 65124, Pescara, Italy.
Sci Rep. 2023 Oct 18;13(1):17793. doi: 10.1038/s41598-023-44243-y.
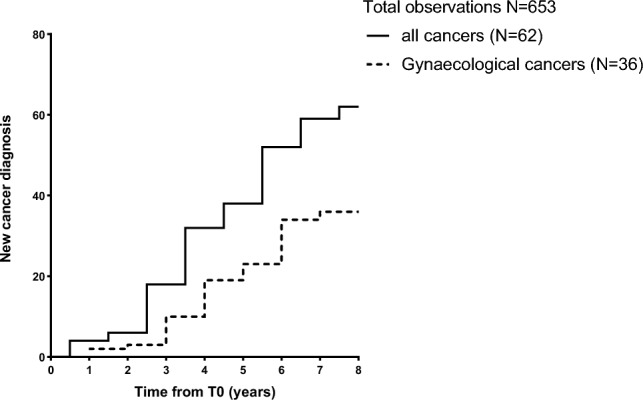
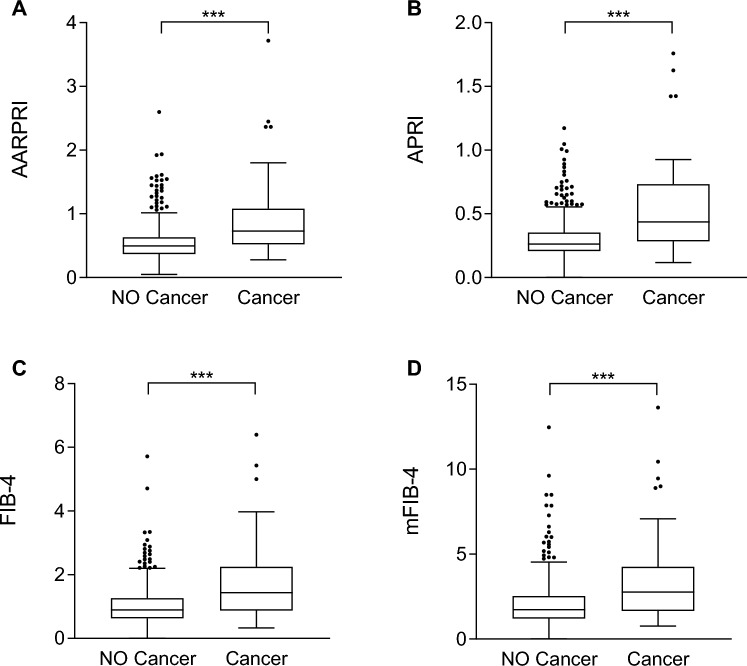
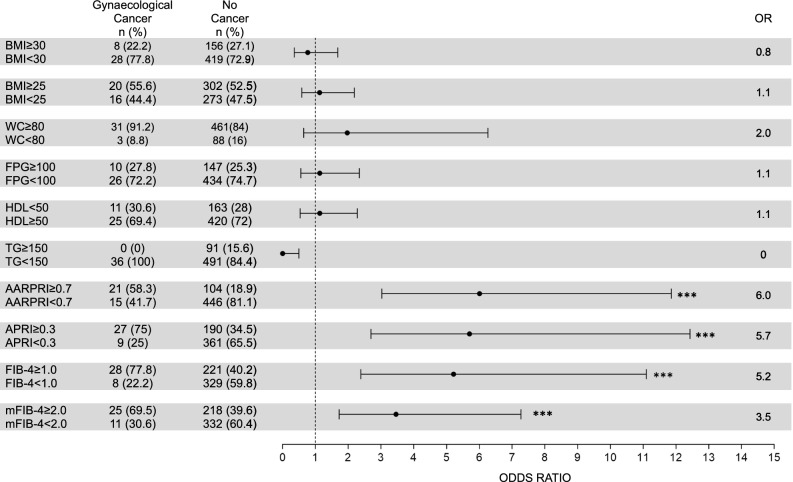
Non-alcoholic fatty liver disease (NAFLD), specifically liver steatosis and fibrosis with steatohepatitis (NASH), is often associated with visceral adiposopathy, whose pathogenetic features have been proposed as tumorigenic triggers. We performed a prospective analysis in 653 metabolic women to reveal any conditions that may predict and concur to cancer development during a 8-years period of follow-up. Among clinical and biochemical variables, only AST and non-invasive liver fibrosis scores (AARPRI, APRI, FIB-4, mFIB4) significantly distinguished cancer-developer women (n = 62, 9.5%) from those who did not develop cancer (p < 0.001). In ROC analysis, these scores also showed good sensitivity and specificity in differentiating women who developed cancer (all p < 0.001). We then calculated OR for these indexes finding that increased AARPRI was associated with the highest risk (OR = 6, p < 0.001) of gynaecological cancers development. We further validated these cut-off values in women who had developed other types of cancer, confirming that AARPRI is able to identify the risk for cancer development (OR = 5, p < 0.001). Our findings support the hypothesis that NAFLD, more than obesity per se, is directly associated with the clinical and pathogenic metabolic scenario of gynaecological cancers and encourage the use of liver fibrosis indexes to detect risk of cancer onset in women. Preventing adiposopathy and NAFLD through lifestyle and therapies may represent an instrumental strategy for cancer prevention and/or co-treatment in oncology.
非酒精性脂肪性肝病(NAFLD),特别是伴有脂肪性肝炎的肝脂肪变性和纤维化(NASH),常与内脏脂肪病有关,其发病特征被认为是致癌的触发因素。我们对 653 名代谢异常的女性进行了前瞻性分析,以揭示在 8 年的随访期间可能预测和并发癌症发展的任何情况。在临床和生化变量中,只有 AST 和非侵入性肝纤维化评分(AARPRI、APRI、FIB-4、mFIB4)显著区分了发生癌症的女性(n=62,9.5%)和未发生癌症的女性(p<0.001)。在 ROC 分析中,这些评分在区分发生癌症的女性方面也显示出良好的敏感性和特异性(均 p<0.001)。然后,我们计算了这些指标的 OR,发现 AARPRI 增加与妇科癌症发展的最高风险(OR=6,p<0.001)相关。我们进一步在发生其他类型癌症的女性中验证了这些截止值,证实 AARPRI 能够识别癌症发展的风险(OR=5,p<0.001)。我们的研究结果支持这样一种假设,即与肥胖本身相比,NAFLD 直接与妇科癌症的临床和发病代谢情况相关,并鼓励使用肝纤维化指数来检测女性癌症发病的风险。通过生活方式和治疗预防脂肪病和 NAFLD 可能代表癌症预防和/或肿瘤学联合治疗的一种重要策略。